Post-Mohs Reconstruction Methods of a Combination Dermatologist and Facial Plastic Surgeon Practice
Omeed Memar1, Benjamin Caughlin2,3,4,5
2.Department of Surgery, Division of Otolaryngology, John H. Stroger, Jr. Hospital of Cook County, Chicago, Illinois,
3.Division of Facial Plastic and Reconstructive Surgery, Jesse Brown VAMC, Chicago, Illinois,
4.Division of Facial Plastic and Reconstructive Surgery, University of Illinois Health Hospital System, Chicago, IL,
5.Kovak Cosmetic Center, Oakbrook Terrace, Illinois
Citation : Memar O, Caughlin B. Post-Mohs Reconstruction Methods of a Combination Dermatologist and Facial Plastic Surgeon Practice. Clinic Res Dermatol 2018;1(1):1-4.
Objective: To determine the benefits of closing post-Mohs defects by both a Mohs surgeon and facial plastic surgeon. Skin cancer is the most common cancer in the United States of America. It is treated by removal. Certain forms of skin cancer are removed using Mohs micrographic surgery. The resulting wound can be large at times. The majority of the reconstruction is handled by the Mohs surgeons.
Methods: We presented 358 Mohs closures that were done at a practice where a combined surgical team of a Mohs surgeon and Facial plastic surgeon operated together in a team as opposed to individually.
Results: We find that this combination provided more flap closures, while previous publications had shown that Mohs surgeons more often close with a primary closure. Furthermore, this combination surgical team provided a wider range of closure techniques than closure done by Mohs surgeons.
Conclusion: This is the first publication presenting a large number of post-Mohs closures that were reconstructed by a combined Mohs surgeon and facial plastic surgeon. The significance is that this a wider range of closure techniques and a greater number of skilled hands reconstructing, since two surgeons is greater than one.
Combined closure, facial plastic surgeon, Mohs micrographic surgery,dermatology
INTRODUCTION
Mohs micrographic surgery is a very accurate method in the resection of contiguous tumors[1]. Tumor size is the main factor involved in the final defect size[2]. Scalp, face, and neck are the most common locations Mohs surgery is performed[3]. Dr. Frederick Mohs, the inventor of the procedure, allowed most post-Mohs wounds to heal secondarily,[4] however today, the defects are reconstructed; the reconstruction is performed by the Mohs surgeons, i.e. commonly dermatologists,[5] in the great majority of cases[6]. The role of the plastic surgeon in skin cancer management is evolving[7]. There is scant literature on collaborative closures, where both Mohs surgeon and plastic surgeons perform the closure.
We present patients from a practice where both a Mohs surgeon and a Plastic Surgeon operated together. We present the methods of reconstruction selected by a Mohs and Facial Plastic surgeon duel practice in the association between the number of stages, tumor type, and anatomic location.
METHODS
Skin cancer patients treated at Academic Dermatology and Skin Cancer Institute were selected. At this clinic, the patients were treated by both the Mohs surgeon and Plastic surgeon. 358 consecutive patients were selected. The patients were treated for BCC, SCC, melanoma in situ, sebaceous carcinoma, and basosquamous carcinoma. Only patients treated for lesions on the head and neck were included.
For each Mohs case, data on the age of the patient, tumor type, location of tumor, tumor diameter size, the number of Mohs stages needed to clear the margins, and the final defect diameter size were recorded.
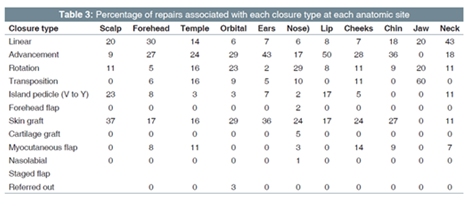
Furthermore, the methods employed in the reconstruction of the remaining defect were recorder. These methods included, primary closure (including complex layered closure), advancement flap, rotation flap, transposition flap, island pedicled flap, forehead flap, skin graft, use of cartilage graft, myocutaneous flap, staged melolabial flap, secondary intention, or outside referral to other plastic surgeons.
The statistical data were completed as previously described[6].
RESULTS
Our analysis showed that the number of Mohs stages associated with different repairs was statistically significantly different (ANOVA, P < 0.001). The descriptive numbers [Table 1] show that linear repairs were associated with the least number of Mohs stages, about 2.7. The paramedian forehead flap was associated with the greatest number of Mohs stages. The use of cartilage grafts was associated with a mean of 4 Mohs stages.
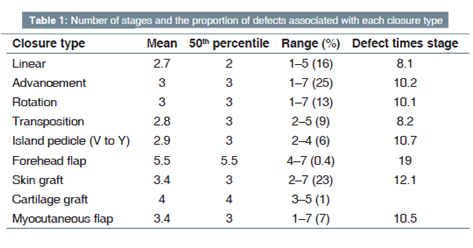
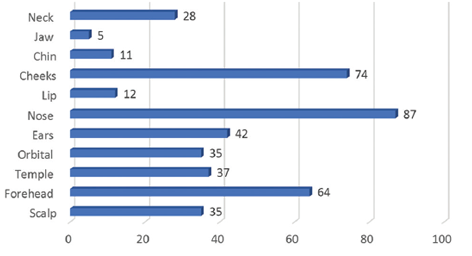
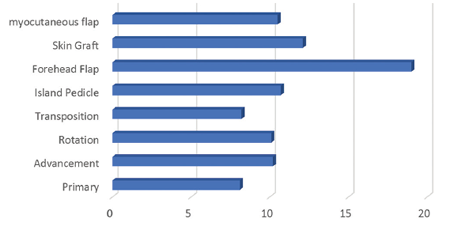
In total numbers, nose, cheek, and forehead were the most common location of defects [Figure 1]. Analysis reveals, when the number of Mohs stages is multiplied by the widest diameter of a post-Mohs defect, the smallest number is the linear closure, followed by transposition flaps, rotation flap, advancement flap, myocutaneous flap, island pedicle flap, and full-thickness skin graft, and the largest number is the forehead flap. Therefore, wound size multiplied by Mohs stage has a distinctive closure breakdown choice. [Figure 2] Primary closure had the lowest Stage X Defect number, followed by transposition flap, while the paramedian forehead flap had the highest number.
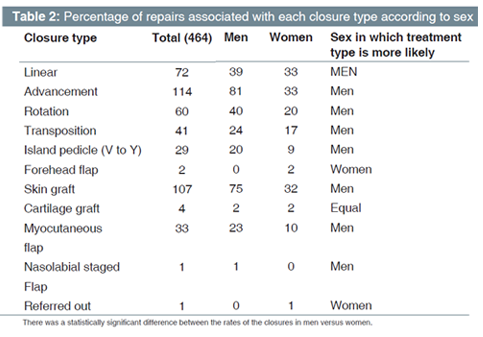
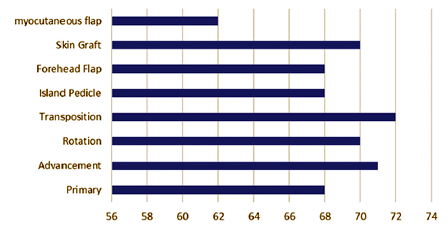
More detailed analysis of the population showed differences in sex versus closure and age versus closure. Table 2 shows that most closures in our combined practice were done on men, and women were more likely to get paramedian forehead flap or be referred out for closure. Figure 3 shows that the youngest population was more likely to get a myofasciocutaneous flap (mean age 62), while transposition flaps were done on the more elderly (mean age 72). On the nose, the most common closure was a rotation flap. On the cheek, advancement flap was most common, and on the forehead, the linear closure was most commonly used.
DISCUSSION
Our study is the first of its kind that shows the value of Mohs closures done by both a Mohs surgeon and facial plastic surgeon. Mohs surgeons do the majority of post-Mohs reconstruction, or they refer out the tough cases. Here, we have shown a practice where the Mohs surgeon and facial plastic surgeon do the closures together. There are a number of benefits and drawbacks. The benefits include a wider range of closure techniques. Second, two set of surgeon's hands can only benefit the patient and increase the efficiency of closure. We had more average layers than the Alam et al. study. The need to refer out for closures is reduced, as shown, we referred 1 patient, which amounted to 3% of peri-ocular defects, while dermatologists referred out 23.5% of the periocular defects, and 10% of their overall defects[6].
We did more hair-bearing skin grafts on the scalp, while dermatologists tend to do more primary closures. This is a technique, where the graft is taken from the posterior scalp. On the temples, we did more advancement flaps, while dermatologists tend to do linear closure. Peri-orbital and ear, we did more advancement flap and skin grafts, while dermatologists closed with primary closure. On the nose, we use a rotation flap, while dermatologists mainly used primary closure. On the cheeks and chin, we used an advancement flap, while they closed primarily. On the jaw, we used transposition flap, while they closed primarily[6].
The drawback of having two surgeons is the coordination in timing for both surgeons to be present and the financial compromise since one cannot double bill for the same closure. However, we feel the ultimate outcome is worth this price, since the patient gets two trained eyes, from different disciplines offering a wider range of closure options.
CONCLUSION
This is the first publication presenting a large number of post-Mohs closures that were reconstructed by a combined Mohs surgeon and facial plastic surgeon. The significance is that this is a wider range of closure techniques and a greater number of skilled hands reconstructing since two surgeons are >1.
ACKNOWLEDGMENTS
All work and statistics done were performed by the authors equally.
REFERENCES
- Kershenovich R, Atzmony L, Reiter O, Lapidoth M, Mimouni D. Trends in the mohs surgery literature: 1994-2013. Dermatol Surg 2017;43:876-80.
- Thomas CL, Lam A, Lam J, Paver R, Storey L, Fernandez-Penas P, et al. Factors affecting choice of repair in mohs micrographic surgery for non-melanoma skin cancer of the head. Australas J Dermatol 2017;58:189-93.
- Reeder VJ, Gustafson CJ, Mireku K, Davis SA, Feldman SR, Pearce DJ, et al. Trends in mohs surgery from 1995 to 2010: An analysis of nationally representative data. Dermatol Surg 2015;41:397-403.
- Mohs F. Chemotherapy: A microscopically controlled method of cancer excision. Arch Surg 1941;42:279-95.
- Kantor J. Dermatologists perform more reconstructive surgery in the medicare population than any other specialist group: A cross-sectional individual-level analysis of medicare volume and specialist type in cutaneous and reconstructive surgery. J Am Acad Dermatol 2018;78:171-30.
- Alam M, Helenowksi IB, Cohen JL, Levy R, Liegeois N, Mafong EA, et al. Association between type of reconstruction after mohs micrographic surgery and surgeon-, patient-, and tumor-specific features: A cross-sectional study. Dermatol Surg 2013;39:51-5.
- Shayan R. The future of skin cancer surgery: What role for plastic surgeons? Aust J Plastic Surg 2018;1:40-5.