Occupational Therapy and Social Skills Training for Enhancing Constructive Engagement of Patients with Schizophrenia: A Review
Viviana Perilli1, Fabrizio Stasolla2, Stefania Maselli1, Isabel Morelli1
2.Telematic University "Giustino Fortunato" of Benevento, Italy.
Citation : Perilli V, Stasolla F, Maselli S, Morelli I. Occupational Therapy and Social Skills Training for Enhancing Constructive Engagement of Patients with Schizophrenia: A Review. Clin Res Psychol 2018;1(1):1-7.
Schizophrenia is a psychiatric illness characterized by a disruption of cognitive, communicative, emotional, social, and occupational functioning.
The objectives of this study were to assess the effectiveness of occupational therapy and social skills training (SST) on the constructive engagement of patients with schizophrenia and to evaluate the suitability of SST on adaptive responding of persons with schizophrenia.
A selective literature review was carried out by retaining some meaningful empirical studies on the use of occupational therapy and social training skills of patients with schizophrenia.
Data showed that both strategies were largely helpful, although few failures occurred. The participants relevantly increased their constructive engagement during intervention phases.
Occupational therapy and SST were useful for enhancing constructive engagement of patients with schizophrenia.
Constructive engagement, occupation therapy, quality of life, schizophrenia, social skills training.
INTRODUCTION
Schizophrenia is a psychiatric condition characterized by a disruption of the cognitive, communicative, emotional, social, and occupational functioning. Hallucinations, delusions, social withdrawal, apathy, and disorganized psychotic symptoms are commonly reported. Growing empirical evidences emphasize the crucial role of psychosocial interventions merged to medical treatments. Thus, psychotic symptoms are significantly reduced, and recovery is relevantly improved, with long-term beneficial outcomes and an arrest of the illness progression [1-3]. Clinicians usually use new and effective strategies and technologies in the treatment of individuals with schizophrenia. For instance, successful systems rely on comprehensiveness and continuity of care. Technologies such as case management and supported employment have their established validity [4,5]. Psychosocial interventions and models of quality of life in schizophrenia are based on the notion that increases in psychosocial functioning will be associated to improvement in subjective experiences, such as self-esteem, fulfillment, and satisfaction [6]. Among behavioral interventions, occupation therapy (OT) and social skills training (SST) are frequently and efficiently implemented [7-10].
OT consists on the use, assessment, and intervention to develop, recover, generalize, and maintain the significant daily activities or occupations of individuals, groups of communities. OT services may include comprehensive evaluation of client's home and other environment (e.g., medical and/or rehabilitative center and workplace), recommendations for adaptive equipment and training in its use, and guidance and education for family members, staff and caregivers. Usually, OT practitioners have a holistic perspective, in which the focus is on adapting the environment to fit the person, and the person is an integral part of the therapy team [11,12].
SST is a collection of strategies aimed at improving the quality of life of patients with schizophrenia. Interpersonal communication, social relationship, and social support are specifically enhanced. Comprehensive programs for schizophrenia patients include basic conversational skills, assertiveness skills, interpersonal problem solving, conflict management skills, friendship and dating skills, work, and vocational skills. Methods basically used in SST refer to modeling, role playing, backward and forward chaining, feedback reinforcement, and corrective feedback. Training is typically conducted in small groups (i.e., 6-10 participants). A session can be collected according to an individual criterion or based on family members because these persons can facilitate and reinforce the acquisition and/or the recovery of the skill. Average persistence of the learning process is about 2 years. Then, it needs a new practice. Research has demonstrated that SST can easily increase social functioning, although it has little effect on risk of relapse [13-15].
The literature on the separated use of OT and SST for promoting adaptive skills of patients with schizophrenia is substantial [16-20]. Review papers on the single use of both are available However, both strategies have been rarely merged [21,22]. Accordingly, the primarily goal of the current review paper is to provide the reader with a concise overview of the literature available in the last two decades on the use of OT and SST for enhancing constructive engagement, independence, self-determination, and adaptive responding of patients with schizophrenia. Some meaningful studies on both strategies were reviewed. Strengths and weaknesses of the retained contributions were emphasized. Implications of the findings were discussed, and some useful guidelines for future research and practice were outlined.
METHODS
A computerized search was performed in SCOPUS. A manual search was includedandmergedascompletion. Schizophrenia, OT, SST, quality of life, constructive engagement, inclusion, independence, and self-determination were used as keywords. Eligibility criteria were (a) at least an empirical contribution, (b) at least a participant with schizophrenia, (c) English language of the paper, and (d) publication year range included between 2000 and 2018. Accordingly, fifteen studies were reviewed, with 1548 participants included. Irrespective of the number of the studies within each category, four studies were concisely described, with the objectives of the interventions, the recruited participants, the procedures, and the mininum results. Two synoptic tabs were added as completion, with the authors of the studies, the selected participants with their chronological age, the adopted strategies, and the outcomes.
LITERATURE REVIEW
As mentioned above, OT is focused on the acquisition and the recovery of daily activities and/or occupation. Thus, through an OT-based intervention, the patient with schizophrenia should be able to independently manage daily functional and/or vocational activities. Furthermore, his/her constructive engagement, positive participation, and adaptive responding should be improved. Accordingly, both families and caregivers' burden should be significantly reduced with beneficial outcomes on the psychological environment. Seven studies were retained in this section with 618 participants involved [Table 1] [23-29].
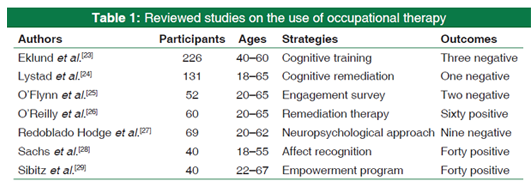
For example, Eklund et al.[23] evaluated the effectiveness of the 16-week Balancing Everyday Life (BEL) program compared to care as usual (CAU) for people with mental illness in specialized and community-based psychiatric services. The main outcomes referred to different features of subjectively assessed everyday activities, in terms of the engagement and satisfaction they bring, balance among activities, and activity level. Secondary outcomes concerned various aspects of well-being and functioning. BEL was a group and activity- based lifestyle program. Active support and mainly standard occupational therapy were embedded in CAU. The BEL group was composed of 133 participants, the CAU group recruited 93 participants. The participants of both the groups completed self-report questionnaires targeting activity and well-being on three occasions, namely (a) at baseline, (b) at the intervention completion (i.e., at 16 weeks), and (c) at a 6-month follow-up. At the same times, a research assistant assessed the participants' level of functioning and symptoms severity. Results showed that BEL group improved more than CAU group from baseline to 16 weeks on primary outcomes in terms of activity engagement, level, and balance. The BEL group also improved more than CAU group from baseline to 16 weeks on secondary outcomes. Specifically, significant differences emerged on symptoms severity and level of functioning. However, no differences were demonstrated between-group on well-being. High intraclass correlations corroborated clustering effects for symptoms severity and level of functioning. Between-group differences were confirmed for activity engagement and level during the 6-month follow-up.
Lystad et al.[24] examined the effects of vocational rehabilitation (VR) to counteract high unemployment rates. The outcomes of cognitive remediation (CR) combined to VR, compared to techniques of cognitive-behavioral therapy (CBT) combined with VR on neurocognition and occupational functioning over a 2-year period. A total of 131 participants underwent an assessment with the MATRICS consensus cognitive battery (MCCB) at baseline, post- treatment (i.e., after 10 months), and follow-up (i.e., 2 years after randomization). Occupational status and number of hours worked were recorded at all assessment points. Both groups improved on several neurocognitive domains. All improvements were in favor of CR group. There was a significant increase in a number of participants working and hours worked in both the groups throughout the intervention period, with no between-group differences. The number of hours worked at follow-up was predicted by change in working memory and the composite score in the CR group. CR-augmented VR improved several domains.Specifically, Verbal Learning and Working Memory, which were critical in the CR intervention increased. The combination of VR and CR or CBT enabled individuals with schizophrenia to attain and maintain work over the time.
O'Reilly et al.[26] carried out a randomized controlled trial to corroborate the suitability of cognitive remediation therapy (CRT) including 60 participants diagnosed with schizophrenia or schizoaffective disorder, who were randomly assigned to one of two conditions, namely (a) CRT with treatment as usual (TAU) or TAU. CRT consisted of 42 individual sessions and 14 group sessions. The primary outcome measure for this study was the change in cognitive functioning using the MCCB. Secondary outcomes included changes in social and occupational functioning, disorganized symptoms, negative symptoms, violence, participation in psychosocial treatment, and recovery. In addition, participants' satisfaction was monitored. Results outlined that cognitive difficulties experienced by schizophrenia spectrum patients were associated with general functioning, ability to benefit from psychosocial intervention, and quality of life. Data positively answered the question whether CRT was an effective intervention strategy for forensic mental health patients. Specifically, it tested whether a representative cohort of patients with schizophrenia or schizoaffective disorder benefited from CRT and whether they were satisfied of the intervention. In addition, a focus on cognitive strategy as a primary treatment had the potential to reduce violence risk in two ways. First, it could help patients who were cognitively impaired benefit from specialized psychosocial programs targeting the risk of violence. Second, it could improve general functioning ability.
Redoblado Hodge et al.[27] assessed a multisite community study, which examined 69 individuals with schizophrenia, who underwent CRT using the Neuropsychological Educational Approach to Remediation (NEAR). Evaluations using the same neuropsychological tests and measure of psychosocial outcome were collected at four-time points: (a) Baseline, (b) before start of active intervention, (c) end of active intervention, and (d) 4 months after the end of active intervention. Dose of antipsychotic medication remains identical throughout the study. After participating in NEAR, patients evinced relevant increasing in verbal and visual memory, sustained attention, and executive functions. The positive effect was confirmed during the 4-month follow-up. The average effect size varied between mild and moderate. Social and occupational outcomes also improved from baseline to post-treatment, which persisted 4 months later. NEAR was effective in improving cognition in patients with schizophrenia in a naturalistic and ecologically valid setting.
A second approach aimed at promoting self-determination, adaptive responding, and the independence of patients with schizophrenia is represented by SST. Psychiatric treatment and rehabilitation are viewed as integrated, seamless approaches focused on restoring and recovering persons with major mental disorders to the higher level of functioning and quality of life. An illustrative example of combined treatment and rehabilitation is the use of pharmacotherapy associated to supported employment, SST, family psychoeducation, assertive community intervention, and integrated programs for persons with psychotic disease. Within this framework, SST pursues the goal of minimizing the symptoms and relapse while maximizing social function. An SST-based intervention would primarily be directed to developing illness management strategies, improving social functioning, and changes in symptoms, as far as they are significantly reduced and considered irrelevant to achieving the objectives of the treatment [30-32]. Eight studies were reviewed in this section, with 930 participants involved [Table 2] [33-40]
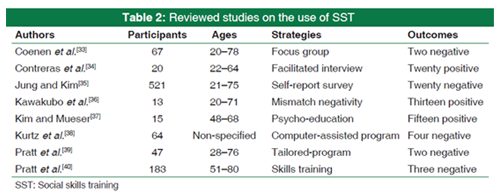
For instance, Coenen et al.[33] carried out a study to determine whether persons with neuropsychiatric disorders experienced a common set of psychosocial difficulties using qualitative data from focus group and individual interviews. The investigation was conducted in five European countries (i.e., Finland, Italy, German, Poland, and Spain), adopting the focus group and individual interviews with persons with nine neuropsychiatric disorders (i.e., dementia, depression, epilepsy, migraine, multiple sclerosis, Parkinson's disease, schizophrenia, stroke, and substance dependence). Digitally recorded sessions were examined using a step-by-step qualitative and quantitative methodology, resulting in the compilation of a common set of psychosocial difficulties using the International Classification of Functioning, Disability, and Health as framework. 67 persons were involved. Most persons with neuropsychiatric disorders experienced problems in emotional functions, sleeping, carrying out a daily routine, working, and interpersonal relationship. 16 of the 33 psychosocial difficulties made-up the common set. The set included mental functions, pain, and issues addressing activities and participation and provided the first evidence for the hypothesis of horizontal epidemiology of psychosocial difficulties in neuropsychiatric disorders.
Contreras et al.[34] explored the subjective experience of 20 participants with schizophrenia undertaking a CR trial. The participants completed a questionnaire-facilitated interview, after being exposed to 20 h of CR. Thematic analysis was then used to identify codes and themes. Accordingly, three themes were identified. Relatively to the reported benefits, all participants found the training to be a positive experience, with 70% having identified cognitive improvements, 45% improved motivation or confidence, and 20% improved social skills. The role of cognitive trainer in being supportive, adaptive, and instructive was consistently indicated as relevant, and most participants positively commented on the group format. Fewer participants observed a transfer to real life settings, with improved social skills, use of cognitive strategies, or features of everyday living reported by 40% of the participants.
Kurtz et al.[37] compared the effects of an extended (i.e., 6 months), standardized, computer-assisted CR intervention, administrated along with a standardized program of SST, with training program (i.e., computer Skills). 64 individuals with schizophrenia recruited from two treatment sites were randomly assigned to one of two conditions, namely (a) CR and (b) SST. Furthermore, they were assessed by blinded raters on neurocognitive measures, performance- based measures of social skill, and rating of psychosocial functioning before and after treatment. Results emphasized that the CR group improved relevantly more in attention, working memory, and empathy than computer skills group. However, no differences emerged between groups on other measures of psychosocial functioning or skills. The findings suggested that CR used in the context of other evidence-based psychosocial interventions (i.e., SST) enhanced working memory in schizophrenia and recommended that this effect would be generalized to improved empathy.
Pratt et al.[39] conducted a pilot study of an individual tailored program to improve community living and health self- management skills in older adults with serious mental illness. The study provided the Helping Older People Experience Success-Individually Tailored (i.e., HOPES) intervention, an adaptation of an empirically supported, manualized, group- based skill training program shown to improve community functioning, psychiatric symptoms, self-efficacy, and receipt of preventive health. HOPES targeted five skill areas:(a) Leisure time and communication, (b) communication,(c) independent living, (d) friendship, and (e) health self- management. 47 adults with serious mental problems (i.e., 38% with schizophrenia and 62% with mood disorders). Trained HOPES coaches assessed participants' skills and functioning and engaged them in shared decision-making to select which curricular areas to receive. Participants were exposed to one HOPES session per week along with a 9-12 months' time period of intervention. The assessment of overall psychosocial functioning and the five skill areas was recorded at baseline, post-intervention, and 3 and 6 months. Results evinced that participants with baseline impairments in overall functioning and in each of the skill areas targeted by the program significantly improved their performance and increased the related outcome measures. Selection of specific HOPES curriculum was not correlated with the level of impairment in associated skill areas at baseline, but participants with more impairments overall choose and completed more curriculum modules.
DISCUSSION
Data of the reviewed studies confirmed the effectiveness and the suitability of both intervention strategies (i.e., OT and SST) for promoting independence and self-determination of patients with schizophrenia spectrum and severe psychotic disorders. The results were largely positive, although few failures occurred (i.e., 3%). The current review emphasized that the performance of the participants was significantly increased during the intervention periods, and their constructive engagement was enhanced. Participants' adaptive responding improved and their psychotic features were relevantly reduced accordingly. The learning process was maintained over the time and generalized across settings. These data were supported by previous findings [41-45] and suggested the following considerations.
First, OT and SST were effective for the acquisition and the recovery of daily functional activities. People with schizophreniaspectrumlearnedtofunctionallyusetheproposed programs for improving their performance and reducing their withdrawal, isolation, and passivity. The independence and self-determination of the participants were enhanced. One may argue that both approaches may be considered as valid educational, psychological, and rehabilitative resources for emphasizing the participants' active role toward the environment in daily settings. Accordingly, caregivers' and families' burden was significantly reduced. Social interactions and communication skills were favorably acquired [2,18,46].
Second, both strategies can be viewed as affordable for daily contexts. Both families and caregivers may have relatively cheap, not expensive solutions (i.e., no more than 1000 USD), even if technological supports and/or computerized interventions were adopted for daily life. Similarly, a tailored and individualized solution profitably fitted the participants' needs with beneficial effects on their performance. Thus, by being adequately rewarded and motivated with individualized options, the participants were positively occupied, and the learning process was fostered [47,48].
Third, participants with schizophrenia spectrum were constructively engaged. That is, by designing an user- tailored rehabilitative strategy, they were focalized on new adaptive skills. Their psychotic problems and/or challenging behaviors were redirected toward new adaptive responding and functional social skills (e.g., self-management and/or communication opportunities). One may argue that, rather than looking for self-stimulation, people with schizophrenia were efficiently taught to performing new and adaptive behaviors with positive outcomes for themselves, families, and caregivers in daily contexts [49,50].
Fourth, the learning process was consolidated over the time. Thus, even if the intervention was suspended, participants maintained their levels of performance and generalized it across settings, tasks, and caregivers. One may argue that the causal association between behavioral responses and environmental consequences were empirically demonstrated to be solid. In other words, the selected behavioral responses did not require a high cost as efforts, the retained activities were rewarded, and the screened stimulation was highly motivating. The learning principles were corroborated.[8,51]
Fifth, few failures occurred (i.e., 3% of the recruited participants). Three basic explanations might be putted forward. First, the selected behavioral response required an excessive effort to be performed. Second, the selected functional activities were not sufficiently meaningful for the selected participant. Third, the positively stimulation used was not adequately motivating. With regard to the first point, new extensions of the reviewed studies should deal with targeting new and easily adaptive responses already available in the persons' behavioral repertoire. With regard to the second point, further investigations should outline updated solutions suitable and feasible for both financial and human resources. With regard to the third point, researchers and clinicians should constantly modify the screened stimulation as to avoid satiation and saturation phenomena [52].
Concluding, in light of the above, new research perspectives within this framework should be focused on (a) new extensions of OT and SST strategies including new participants with schizophrenia spectrum and/or different psychotic disorders, (b) further updating of the technological solution available and/or learning strategies within this specific topic, (c) the inclusion of preference check assessment by the participants involved, and (d) social validation procedures for recruiting external raters to corroborating social and clinical validity of the implemented programs.
REFERENCES
- Armijo J, Mendez E, Morales R, Schilling S, Castro A, Alvarado R, et al. Efficacy of community treatments for schizophrenia and other psychotic disorders: A literature review. Front Psychiatry 2013;4:116.
- Chien WT, Leung SF, Yeung FK, Wong WK. Current approaches to treatments for schizophrenia spectrum disorders, Part II: Psychosocial interventions and patient-focused perspectives in psychiatric care. Neuropsychiatr Dis Treat 2013;9:1463-81.
- Spurrell M. Should women be a special case when it comes to services for psychosis? Ment Health Today 2008;12:23-6.
- Gunatilake S, Ananth J, Parameswaran S, Brown S, Silva W. Rehabilitation of schizophrenic patients. Curr Pharm Des 2004;10:2277-88.
- Nicol MM, Robertson L, Connaughton JA. Life skills programmes for chronic mental illnesses. Cochrane Database Syst Rev 2000;2:CD000381.
- Vaccaro JV, Young AS, Glynn S. Community-based care of individuals with schizophrenia. Combining psychosocial and pharmacologic therapies. Psychiatr Clin North Am 1993;16:387-99.
- McClellan J. Psychosis in children and adolescents. J Am Acad Child Adolesc Psychiatry 2018;57:308-12.
- Palumbo D, Patriarca S, Pietrafesa D, Merlotti E, Galderisi S. Management of schizophrenia: Current research and development of new strategies. Minerva Psichiatr 2016;57:134-50.
- Vass E, Fekete Z, Simon V, Simon L. Interventions for the treatment of theory of mind deficits in schizophrenia: Systematic literature review. Psychiatry Res 2018;267:37-47.
- Javed A, Charles A. The importance of social cognition in improving functional outcomes in schizophrenia. Front Psychiatry 2018;9:157.
- Granholm E, Holden J, Worley M. Improvement in negative symptoms and functioning in cognitive-behavioral social skills training for schizophrenia: Mediation by defeatist performance attitudes and asocial beliefs. Schizophr Bull 2018;44:653-61.
- Granholm E, Harvey PD. Social skills training for negative symptoms of schizophrenia. Schizophr Bull 2018;44:472-4.
- Turner DT, McGlanaghy E, Cuijpers P, van der Gaag M, Karyotaki E, MacBeth A, et al. A meta-analysis of social skills training and related interventions for psychosis. Schizophr Bull 2018;44:475-91.
- Gordon A, Davis PJ, Patterson S, Pepping CA, Scott JG, Salter K, et al. A randomized waitlist control community study of social cognition and interaction training for people with schizophrenia. Br J Clin Psychol 2018;57:116-30.
- Sahoo S, Padhy SK, Singla N, Singh A. Psychosis in a child with atypical autism: A Case report and a brief review of the association of psychosis and autism. Innov Clin Neurosci 2018;15:33-6.
- Dziwota E, Stepulak MZ, Wloszczak-Szubzda A, Olajossy M. Social functioning and the quality of life of patients diagnosed with schizophrenia. Ann Agric Environ Med 2018;25:50-5.
- Rose A, Vinogradov S, Fisher M, Green MF, Ventura J, Hooker C, et al. Randomized controlled trial of computer- based treatment of social cognition in schizophrenia: The TRuSST trial protocol. BMC Psychiatry 2015;15:142.
- Velligan D, Maples N, Roberts DL, Medellin EM. Integrated psychosocial treatment for negative symptoms. Am J Psychiatr Rehabil 2014;17:1-19.
- Bembry JX, Zentgraf S, Baffour T. Social skills training through poetry therapy: A group intervention with schizophrenic patients. J Poetry Ther 2013;26:73-82.
- Ricarte JJ, Hernandez-Viadel JV, Latorre JM, Ros L. Effects of event-specific memory training on autobiographical memory retrieval and depressive symptoms in schizophrenic patients. J Behav Ther Exp Psychiatry 2012;43:S12-20.
- Wolwer W, Frommann N. Social-cognitive remediation in schizophrenia: Generalization of effects of the training of affect recognition (TAR). Schizophr Bull 2011;37 Suppl 2:S63-70.
- Emsley R, Chiliza B, Asmal L, Lehloenya K. The concepts of remission and recovery in schizophrenia. Curr Opin Psychiatry 2011;24:114-21.
- Eklund M, Tjornstrand C, Sandlund M, Argentzell E. Effectiveness of balancing everyday life (BEL) versus standard occupational therapy for activity engagement and functioning among people with mental illness - A cluster RCT study. BMC Psychiatry 2017;17:363.
- Lystad JU, Falkum E, Haaland Vo, Bull H, Evensen S, McGurk SR, et al. Cognitive remediation and occupational outcome in schizophrenia spectrum disorders: A 2 year follow-up study. Schizophr Res 2017;185:122-9.
- O'Flynn P, O'Regan R, O'Reilly K, Kennedy HG. Predictors of quality of life among inpatients in forensic mental health: Implications for occupational therapists. BMC Psychiatry 2018;18:16.
- O'Reilly K, Donohoe G, O'Sullivan D, Coyle C, Mullaney R, O'Connell P, et al. Study protocol: A randomised controlled trial of cognitive remediation for a national cohort of forensic mental health patients with schizophrenia or schizoaffective disorder. BMC Psychiatry. 2016;16:5.
- Hodge MA, Siciliano D, Withey P, Moss B, Moore G, Judd G, et al. A randomized controlled trial of cognitive remediation in schizophrenia. Schizophr Bull 2010;36:419-27.
- Sachs G, Winklbaur B, Jagsch R, Lasser I, Kryspin-Exner I, Frommann N, et al. Training of affect recognition (TAR) in schizophrenia - impact on functional outcome. Schizophr Res 2012;138:262-7.
- Sibitz I, Provaznikova K, Lipp M, Lakeman R, Amering M. The impact of recovery-oriented day clinic treatment on internalized stigma: Preliminary report. Psychiatry Res 2013;209:326-32.
- Bryce S, Warren N, Ponsford J, Rossell S, Lee S. Understanding the lived experience of cognitive remediation in schizophrenia: A qualitative comparison with an active control. Psychiatr Rehabil J 2018.
- Brooke-Sumner C, Petersen I, Asher L, Mall S, Egbe CO, Lund C, et al. Systematic review of feasibility and acceptability of psychosocial interventions for schizophrenia in low and middle income countries. BMC Psychiatry 2015;15:19.
- Carbon M, Correll CU. Thinking and acting beyond the positive: The role of the cognitive and negative symptoms in schizophrenia. CNS Spectr 2014;19 Suppl 1:38-52.
- Coenen M, Cabello M, Umlauf S, Ayuso-Mateos JL, Anczewska M, Tourunen J, et al. Psychosocial difficulties from the perspective of persons with neuropsychiatric disorders. Disabil Rehabil 2016;38:1134-45.
- Contreras NA, Lee S, Tan EJ, Castle DJ, Rossell SL. How is cognitive remediation training perceived by people with schizophrenia? A qualitative study examining personal experiences. J Ment Health 2016;25:260-6.
- Jung SH, Kim HJ. Perceived stigma and quality of life of individuals diagnosed with schizophrenia and receiving psychiatric rehabilitation services: A comparison between the clubhouse model and a rehabilitation skills training model in South Korea. Psychiatr Rehabil J 2012;35:460-5.
- Kawakubo Y, Kamio S, Nose T, Iwanami A, Nakagome K, Fukuda M, et al. Phonetic mismatch negativity predicts social skills acquisition in schizophrenia. Psychiatry Res 2007;152:261-5.
- Kim C, Mueser KT. The effects of social skills training vs. psychoeducation on negative attitudes of mothers of persons with schizophrenia: A Pilot study. Psychiatry Investig 2011;8:107-12.
- Kurtz MM, Mueser KT, Thime WR, Corbera S, Wexler BE. Social skills training and computer-assisted cognitive remediation in schizophrenia. Schizophr Res 2015;162:35-41.
- Pratt SI, Mueser KT, Wolfe R, Santos MM, Bartels SJ. One size doesn't fit all: A trial of individually tailored skills training. Psychiatr Rehabil J 2017;40:380-6.
- Pratt SI, Mueser KT, Bartels SJ, Wolfe R. The impact of skills training on cognitive functioning in older people with serious mental illness. Am J Geriatr Psychiatry 2013;21:242-50.
- Biagianti B, Fisher M, Howard L, Rowlands A, Vinogradov S, Woolley J, et al. Feasibility and preliminary efficacy of remotely delivering cognitive training to people with schizophrenia using tablets. Schizophr Res Cogn 2017;10:7-14.
- Ikebuchi E, Sato S, Yamaguchi S, Shimodaira M, Taneda A, Hatsuse N, et al. Does improvement of cognitive functioning by cognitive remediation therapy effect work outcomes in severe mental illness? A secondary analysis of a randomized controlled trial. Psychiatry Clin Neurosci 2017;71:301-8.
- Kang R, Wu Y, Li Z, Jiang J, Gao Q, Yu Y, et al. Effect of community-based social skills training and tai-chi exercise on outcomesinpatientswithchronicschizophrenia:A Randomized, one-year study. Psychopathology 2016;49:345-55.
- Even C, Bosser A, Ferreira JF, Buche C, Stephan F, Cavazza M, Lisetti C. Supporting social skills rehabilitation with virtual storytelling. In: Proceedings of the 29th International Florida Artificial Intelligence Research Society Conference, FLAIRS 2016; 2016. p. 329-34.
- Engh JA, Andersen E, Holmen TL, Martinsen EW, Mordal J, Morken G, et al. Effects of high-intensity aerobic exercise on psychotic symptoms and neurocognition in outpatients with schizophrenia: Study protocol for a randomized controlled trial. Trials 2015;16:557.
- Forester BP, Dukoff R. Recognition and management of late- life psychosis. Prim Psychiatry. 2004:48:51-5.
- Rus-Calafell M, Garety P, Sason E, Craig TJ, Valmaggia LR. Virtual reality in the assessment and treatment of psychosis: A systematic review of its utility, acceptability and effectiveness. Psychol Med 2018;48:362-91.
- Kern RS, Zarate R, Glynn SM, Turner LR, Smith KM, Mitchell SS, et al. Improving work outcome in supported employment for serious mental illness: Results from 2 independent studies of errorless learning. Schizophr Bull 2018;44:38-45.
- Solomon P, Alexander L, Uhl S. The relationship of case managers' expressed emotion to clients' outcomes. Soc Psychiatry Psychiatr Epidemiol 2010;45:165-74.
- McQuaid JR, Granholm E, McClure FS, Roepke S, Pedrelli P, Patterson TL, et al. Development of an integrated cognitive- behavioral and social skills training intervention for older patients with schizophrenia. J Psychother Pract Res 2000;9:149-56.
- Singh U, Sweta K, Kiran M. Efficacy of occupational therapy with supportive techniques on social and occupational functioning among person with schizophrenia. Int J Psychosoc Rehab 2017;21:67-74.
- Stasolla F, Perilli V. Microswitch-based programs (MBP) to promote communication, occupation, and leisure skills for children with multiple disabilities: A literature overview. In: Silton N, editor. Recent Advances in Assistive Technologies to Support Children with Developmental Disorders. Hershey: IGI Global; 2015. p. 195-216.