Uncoiling the Tightening Obesity Spiral
Robert L. Cucin
Citation : Cucin RL. Uncoiling the Tightening Obesity Spiral. Clin Res Diab Endocrinol 2018;1(2):1-5.
While an underweight prevalence was once more than twice that of obesity, now more people are obese than underweight. Obesity is one of the leading causes of preventable death in the world. There are an estimated 2,100,000,000 obese people worldwide and that number is forecast to grow to 51% of the world's population by 2030. Escalating obesity-related disease costs threaten to bankrupt the world's health-care systems.
The author reviews some of the causes for the increasing prevalence of this disease, identifies opportunities to intervene to prevent its progression, and discusses possible methods that may avert further increase in the overall prevalence of obesity in the general population.
2,100,000,000 people or nearly 30% of all people about the globe are obese with the U.S. population being the most obese. Not a single nation has succeeded in reducing obesity rates [1]. Although some models suggest obesity may level off 42%, linear trends forecast 51% of the world's population to be obese by 2030 [2]. Obesity-related diseases include gastric reflux, sleep apnea, hypertension, hyperlipidemia, autoimmune diseases and cancer, heart disease, strokes, and most significantly type 2 Diabetes mellitus. The McKinsey Global Institute estimated worldwide annual obesity-related disease costs reached $2,000,000,000. Annual growth with increasing prevalence threatens to bankrupt national health-care systems [3].
The WHO recognized obesity as a disease in 1997. In 2004, obesity was officially classified as a disease by the U.S. Centers for Medicare and Medicaid Services (CMS). The AMA followed suit in 2013, thus removing a major barrier to access to medical treatment for obese patients in the U.S. In 2006, and again in 2012, CMS expanded coverage to include more types of devices and procedures. While CMS pays for only approximately 20% of bariatric procedures for obesity, it sets the standard for all U.S. insurance companies.
Clinical data about obesity-related comorbidities sparked governmental interest in obesity. The U.S. regulatory environment for obesity companies is favorable with access to the expedited access pathway. The Food and Drug Administration (FDA) enacted a benefit-risk paradigm for the clinical trial design of obesity devices and is supportive of advancing new technologies for obesity-related devices and procedures. The U.S. President-elect Donald Trump has expressed a willingness to further loosen FDA policy.
In the vast majority of circumstances, diet and counseling are less successful than weight loss surgery as long-term solutions [4,5]. and successful treatment requires a multidisciplinary approach [6]. However, in spite of the increasing obesity problem, the number of bariatric surgeries performed annually remains limited to a very small portion of the afflicted population.
Established surgical options are either restrictive or bypass in nature. These surgeries involve cutting into the bowel, rearranging the body's alimentary plumbing, or leaving behind a foreign body to force the patient to eat less, or make food leave the body incompletely digested with the potential of creating nutritional cripples. The number of bariatric surgeries has plateaued with annual costs exceeding $1,500,000,000 [7] and was estimated at approximately 196,000 for 2015 by the American Society for Metabolic and Bariatric Surgery (ASMB) with Roux-en-Y and gastric banding losing popularity in favor of gastric sleeves. ASMB reported revisions have more than doubled between 2011 and 2015 and comprise almost 14% of all such surgeries [8]. Although socioeconomic inequities undoubtedly affect these numbers, this suggested low plateau evidence patient and physician dissatisfaction with the costs, risks, and long-term sequelae of current surgical options, reserving surgical intervention for those more severely affected.
Following funding infusions for product development to meet this growing unmet need, multiple technologies have recently attained the U.S. FDA. Premarket approval or are on the verge of doing so [9,10]. These devices and procedures involve novel approaches and provide lower cost, less invasive solutions. They may be grouped into those which will be introduced as temporary diet training aides and those with the potential of being a more permanent solution.
LAP-BAND® (Apollo Endosurgery) is legacy adjustable gastric band that is a minimally invasive laparoscopic weight loss device with both FDA approval and broad-based insurance coverage. However, LAP-BAND®, which is approved for long-term use, has a declining market share due to patients not losing weight, regaining weight lost, significant revisions or complications, [11] or patients not liking draconian portion limits.
The FDA has approved the Orbera Intragastric Balloon System (Apollo Endosurgery) and the ReShape Integrated Dual Balloon System (ReShape Medical) for up to 6 month's use in adults with a body mass index of 30-40 who have not been able to maintain weight loss with a weight loss program and, for ReShape, who have at least one obesity-related comorbidity [12,13]. Similar products such as Satisphere™ (Endosphere) are proceeding with safety studies. Nausea and vomiting experienced by some patients and the slim possibility of the 35% fatal Boerhaave's syndrome may hinder acceptance [14,15]. Furthermore, the stomach is likely to dilate around the device countering its volume-filling effect and leading patients to eat more to be satiated after removal of these temporary devices, regain any lost weight, and possibly be worse off than before the procedure.
Temporary malabsorptive alternatives that may remain in place no more than 12 months include intraluminal shunts such as Endobarrier™ (GI Dynamics) and TIPS™ (BAROnova) [16]. Safety studies of the former for its PMA have been completed and safety studies for the latter are in process. Since any internal shunt to cause food to bypass digestive enzymes will not peristalse like normal bowel, shunts will eventually occlude and need to be replaced or removed [17]. Furthermore, compensatory hypertrophy of distal intestinal villi may reduce efficacy and possibly leave the patient worse off after removal.
Fresh approaches approved for long-term use include attempts to stimulate CN X to induce satiety or emptying. These include Abiliti™ (IntraPace) and VBLOC™ (EnteroMedics). The Maestro rechargeable system for VBLOCK just received approval [18]. These electrostimulation devices suffer not only from their high costs (approximately $20,000 USD) and the necessity of nightly recharging but also from the fact that they can give rise to foreign body complications. The brain's neuroplasticity also makes some degree of habituation likely to lessen long-term efficacy.
In the past decade, we have learned that it is the visceral fat within the abdomen that is responsible for all the morbidity associated with obesity - sleep apnea and gastric reflux simply by bulk, and type 2 diabetes and hypertension, autoimmune diseases, and cancers by virtue of the cytokines it secretes [19,20]. Omental fat is one location for this fat. Removing the omentum in conjunction with a LAP-BAND® procedure has produced an additive beneficial effect [21,22]. Omentectomy has also been shown to have an added beneficial effect when carried out in conjunction with some roux-en-Y bypass procedures, but only if those bypasses were less aggressive and omentectomy was performed more completely [23]. However, even if performed laparoscopically, omentectomy is not a totally benign procedure.
Up until now, it was not safe or efficient to remove the visceral fat in the mesentery of the small bowel that endocrinologists and gastroenterologists believe may be more metabolically active [24]. The thickness of this mesentery has been shown to be directly correlated not only to the severity of metabolic disease [25] but also to the intimal thickening of patient's carotid arteries, providing a clear-cut indicator of the likelihood of vascular disease and stroke [26]. Removal of that mesenteric fat safely and efficiently may now be possible.
Using an endoscopic generation of a technology originally developed to facilitate safer and less onerous liposuction (Twin Cannula Assisted Liposuction or "TCAL"), a tube-within-a-tube tissue removal device that does not require the surgeon to actively stroke or reciprocate an aspirating cannula, [27] the endoscopic visceral lipectomy (EVL)® device under development (BioSculpture Technology, Inc.) will permit laparoscopic assessment, of which intraabdominal fat is the most noxious and to safely and efficiently remove it permanently. EVL will not require cutting into the bowel or stomach, rearranging the body's alimentary plumbing, leaving behind a foreign body, or have any danger of creating malabsorption syndromes and nutritional cripples. Clinical testing and regulatory approvals are yet to be obtained. But, if EVL in humans attains postsurgical weight loss and metabolic improvement similar to visceral lipectomy in animals [19,28-30] it holds potential of not only becoming a first-line procedure in the treatment of established metabolic syndrome and Type 2 diabetes but also of significantly widening patient selection to affect the course of the disease.
An obese mother is 5 times more likely to have an obese child [31]. As visceral adiposity starts in utero, this child will be born with a greater proportion of visceral fat [32]. 25% of children in the U.S. are already obese. Opportunities for intervention and a treatment algorithm may be developed pursuant to the model for the tightening spiral of obesity prevalence as depicted in Figure 1.
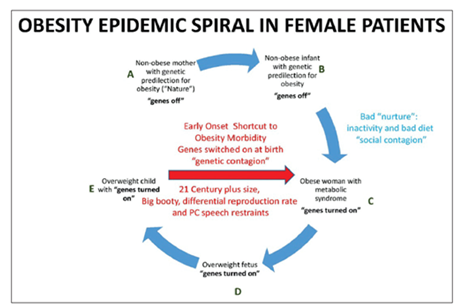
A non-obese mother with or without a genetic predilection for obesity "nature" can enter the cycle at "A" and give birth to a non-obese infant at "B." Obesity is more prevalent among Colored and Hispanic ethnicities (43%). The mother cannot control her genetic predisposition, but she can control the state of the epigenetic switches at the time of conception [33]. If she receives preconception counseling, she can also control whether she chooses to add to her own hard-coded genetic propensities toward obesity in her choice of a similarly genetically disadvantaged mate.
A sedentary lifestyle and bad diet "nurture" and any inherited genetic predilection can convert this child into an obese adolescent with an excess of visceral fat and epigenetic metabolic switches for the noxious visceral fat cytokine factory switched on at "C." Counseling to change dietary and lifestyle as well as any pharmacologic or genetic therapies that may be developed in the future may prevent the child from becoming an obese adult pregnant mother likely to have an obese child. If the obese adolescent becomes an obese pregnant mother at "D," the obesity spiral will tighten until we have an overweight child born with epigenetic obesity switches turned on and an abundance of visceral fat at "E," reentering the cycle at "C" in a tightened spiral shortcut to being an obese pregnant mother herself. However, if we can prevent that mother from being obese at the time of conception and pregnancy, we can uncoil the tightening spiral back to reentry point "A" and reverse this trend to increasing prevalence. Opportunities for pharmacologic, genetic, counseling, or bariatric surgical intervention still exist in the tightened spiral, but the windows for intervention will be narrower and the genetic and epigenetic loads will make success less likely. Any skewing of the population in favor of ethnicities with a higher incidence of Obesity will further increase prevalence.
If EVL proves safe and effective, it may provide a cost-effective means of preventing child from becoming an obese mother when counseling is ineffective or the child is at high risk. From studying the mesenteric fat removed, EVL can allow us to learn whether these patients genetically prone to obesity have numerically more adipocytes present or just adipocytes more full with fat that are actively secreting the adipocytokines that cause metabolic syndrome. . It will also allow us to identify and target the most metabolically active cytokine factories for removal first. The ileal mesentery is a highly suspect offender given its involvement "creeping fat" with such autoimmune diseases as Crohn's disease [34].
An area suggested for the study is whether a father with a family history of obesity will have an additional increased likelihood of an infant being obese if he himself is obese at the time of conception, presumably with his epigenetic obesity switches turned on. If so, this would provide an opportunity on the male side to interrupt the spiral with counseling or EVL for his offspring as well as for his own health.
There is ignorance or general denial by the general population that obesity is a disease [35]. There is still an associated public stigma that obesity is caused by weak willpower or gluttony. There is no general knowledge among the public of genetic transmission of a tendency toward obesity and that, after establishment, obesity is homeostatically maintained by powerful cytokines such as ghrelin, neuropeptide-Y, and resistin causing hunger and preventing insulin from allowing sugar to enter cells to satisfy their metabolic needs. In addition to any inherited genetic propensity, these homeostatic mechanisms are responsible for the frequent failure of diet and counseling.
In conclusion, new medical devices under development such as EVL may permit new less invasive and safer approaches to the obesity problem which allow us to reduce the reverse the trend toward an increasing prevalence of obesity in each subsequent generation. However, success will depend on changes in our lifestyles and diets. More importantly, it will require broad and early public education with counseling to demarcate who is at high risk, when "being overweight" becomes "being obese," and that obesity is a treatable, inheritable disease which shortens and reduces the quality of the lives of those afflicted.
CONFLICTS OF INTEREST
Dr. Cucin serves as C.E.O. of BioSculpture Technology, Inc., a U.S. medical device manufacturer that is developing the EVL® device.
REFERENCES
- Ng M, Fleming T, Robinson M, Thomson B, Graetz N, Margono C, et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980-2013: A systematic analysis for the global burden of disease study 2013. Lancet 2014;384:766-81.
- Finkelstein EA, Khavjou OA, Thompson H, Trogdon JG, Pan L, Sherry B, et al. Obesity and severe obesity forecasts through 2030. Am J Prev Med 2012;42:563-70.
- Dobbs R, Sawers C, Thompson F, Manyika J, Woetzel J, Child P, et al. Overcoming Obesity: An Initial Economic Analysis. Discussion Paper. McKinsey Global Institute; 2014.
- Panosian J, Ding SA, Wewalka M, Simonson DC, Goebel-Fabbri A, Foster K, et al. Physical activity in obese Type 2 diabetes after gastric bypass or medical management. Am J Med 2017;130:83-92.
- Weiner RA. Indications and principles of metabolic surgery. Chirurg 2010;81:379-94.
- Montesi L, El Ghoch M, Brodosi L, Calugi S, Marchesini G, Dalle Grave R, et al. Long-term weight loss maintenance for obesity: A multidisciplinary approach. Diabetes Metab Syndr Obes 2016;9:37-46.
- Livingston EH. The incidence of bariatric surgery has plateaued in the U.S. Am J Surg 2010;200:378-85.
- ASMBS. Estimate of Bariatric Surgery Numbers, 2011-2015. 2016. Available from:
http://www.asmbs.org/resources/ estimate-of-bariatric-surgery-numbers. - Zhu C, Pryor AD. Innovations in bariatric surgery. Surg Technol Int 2015;27:129-35.
- Brethauer SA, Chang J, Galvao Neto M, Greve JW. Gastrointestinal devices for the treatment of Type 2 diabetes. Surg Obes Relat Dis 2016;12:1256-61.
- Altieri MS, Yang J, Telem DA, Meng Z, Frenkel C, Halbert C, et al. Lap band outcomes from 19,221 patients across centers and over a decade within the state of New York. Surg Endosc 2016;30:1725-32.
- Kumar N. Weight loss endoscopy: Development, applications, and current status. World J Gastroenterol 2016;22:7069-79.
- ReShape and orbera-two gastric balloon devices for weight loss. Med Lett Drugs Ther 2015;57:122-3.
- Ponce J, Woodman G, Swain J, Wilson E, English W, Ikramuddin S, et al. The Reduce pivotal trial: A prospective, randomized controlled pivotal trial of a dual intragastric balloon for the treatment of obesity. Surg Obes Relat Dis 2015;11:874-81.
- Yorke E, Switzer NJ, Reso A, Shi X, de Gara C, Birch D, et al. Intragastric balloon for management of severe obesity: A systematic review. Obes Surg 2016;26:2248-54.
- Kumar N. Endoscopic therapy for weight loss: Gastroplasty, duodenal sleeves, intragastric balloons, and aspiration. World J Gastrointest Endosc 2015;7:847-59.
- Rohde U. EndoBarrier gastrointestinal liner. Delineation of underlying mechanisms and clinical effects. Dan Med J 2016;63:B5309.
- Hwang SS, Takata MC, Fujioka K, Fuller W. Update on bariatric surgical procedures and an introduction to the implantable weight loss device: The maestro rechargeable system. Med Devices (Auckl) 2016;9:291-9.
- Muzumdar R, Allison DB, Huffman DM, Ma X, Atzmon G, Einstein FH, et al. Visceral adipose tissue modulates mammalian longevity. Aging Cell 2008;7:438-40.
- Huffman DM, Barzilai N. Role of visceral adipose tissue in aging. Biochim Biophys Acta 2009;1790:1117-23.
- Thorne A, Lonnqvist F, Apelman J, Hellers G, Arner P. A pilot study of long-term effects of a novel obesity treatment: Omentectomy in connection with adjustable gastric banding. Int J Obes Relat Metab Disord 2002;26:193-9.
- Andersson DP, Thorell A, Lofgren P, Wiren M, Toft E, Qvisth V, et al. Omentectomy in addition to gastric bypass surgery and influence on insulin sensitivity: A randomized double blind controlled trial. Clin Nutr 2014;33:991-6.
- Herrera MF, Pantoja JP, Velazquez-Fernandez D, Cabiedes J, Aguilar-Salinas C, Garcia-Garcia E, et al. Potential additional effect of omentectomy on metabolic syndrome, acute-phase reactants, and inflammatory mediators in grade III obese patients undergoing laparoscopic roux-en-Y gastric bypass: A randomized trial. Diabetes Care 2010;33:1413-8.
- Catalano KJ, Stefanovski D, Bergman RN. Critical role of the mesenteric depot versus other intra-abdominal adipose depots in the development of insulin resistance in young rats. Diabetes 2010;59:1416-23.
- Andrade LJ, Melo PR, Parana R, Daltro C. Grading scale of visceral adipose tissue thickness and their relation to the nonalcoholic fatty liver disease. Arq Gastroenterol 2014;51:118-22.
- Liu KH, Chan YL, Chan WB, Chan JC, Chu CW. Mesenteric fat thickness is an independent determinant of metabolic syndrome and identifies subjects with increased carotid intima-media thickness. Diabetes Care 2006;29:379-84.
- Becker DG, Cucin RL Chapter: Powered liposuction. In: Powered Instrumentation in Surgery. San Diego, California: Singular Publishing Group; 2000.
- Huffman DM, Barzilai N. Contribution of adipose tissue to health span and longevity. Interdiscip Top Gerontol 2010;37:1-9.
- Pitombo C, Araujo EP, De Souza CT, Pareja JC, Geloneze B, Velloso LA, et al. Amelioration of diet-induced diabetes mellitus by removal of visceral fat. J Endocrinol 2006;191:699-706.
- Gabriely I, Barzilai N. Surgical removal of visceral adipose tissue: Effects on insulin action. Curr Diab Rep 2003;3:201-6.
- Godfrey KM, Reynolds RM, Prescott SL, Nyirenda M, Jaddoe VW, Eriksson JG, et al. Influence of maternal obesity on the long-term health of offspring. Lancet Diabetes Endocrinol 2017;5:53-64.
- Jovanovic-Peterson L, Crues J, Durak E, Peterson CM. Magnetic resonance imaging in pregnancies complicated by gestational diabetes predicts infant birthweight ratio and neonatal morbidity. Am J Perinatol 1993;10:432-7.
- Adamo KB, Ferraro ZM, Brett KE. Can we modify the intrauterine environment to halt the intergenerational cycle of obesity? Int J Environ Res Public Health 2012;9:1263-307.
- Kredel LI, Siegmund B. Adipose-tissue and intestinal inflammation-visceral obesity and creeping fat. Front Immunol 2014;5:462.
- Oksel E, Gunduzoglu NC, Topcu S. The perception of obese persons: Cross cultural considerations. Holist Nurs Pract 2015;29:225-31