Helicobacter pylori Frequency in Polycythemia Vera Patients without Dyspeptic Complaints
Emre Gezer1, Sinem Namdaroglu2, Ozlem Ergin3, Oktay Bilgir2
2. Department of Hematology, Izmir Bozyaka Training and Research Hospital, Izmir, Turkey.
3. Department of Microbiology, Izmir Bozyaka Training and Research Hospital, Izmir, Turkey.
Citation: Gezer E, Namdaroglu S, Ergin O, Bilgir O. Helicobacter pylori Frequency in Polycythemia Vera Patients without Dyspeptic Complaints. Clin Res Hematol 2018;1(1):1-7.
In polycythemia vera (PV) patients, peptic ulcer and gastroduodenal erosions are more common than the general population, but there are insufficient data on the frequency of Helicobacter pylori (HP) and its role in etiopathogenesis. In this study, we aimed to compare the prevalence of HP infection in PV patients without dyspeptic complaints with a healthy control group without dyspeptic complaints.
Fifty patients with PV without dyspeptic complaints and 50 controls without dyspeptic complaints were enrolled in this study after informed consent obtained. Stool samples of selected patients were analyzed using HP stool antigen test (True Line®).
There was surprisingly striking difference between HP prevalence in PV patients without dyspeptic complaints and asymptomatic healthy controls (64% vs. 2%) (P < 0.05). There was no significant relationship found between HP presence and age, gender, treatment modalities, complete blood count, positivity of JAK2 V617F, serum erythropoietin level, and splenomegaly in PV patients (P > 0.05).
As the susceptibility of HP infections in PV patients are higher, it is recommended to have close surveillance of these patients by screening HP presence. In addition, when HP positivity is determined, the eradication of HP is essential to prevent possible future gastrointestinal lesions in patients with PV.
Helicobacter pylori, Helicobacter pylori stool antigen test, Polycythemia vera
INTRODUCTION
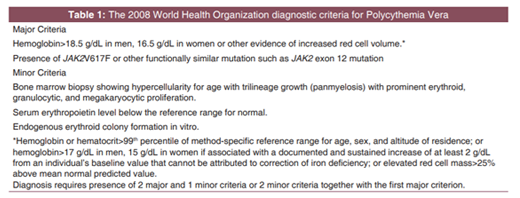
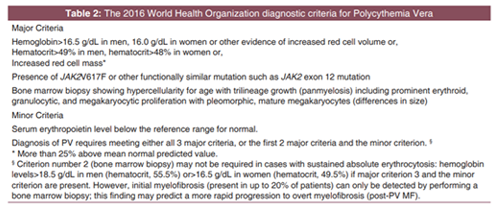
Polycythemia vera (PV) is a clonal, progressive myeloproliferative neoplasm characterized by erythrocytosis, leukocytosis, thrombocytosis, and splenomegaly. The median age at diagnosis is approximately 60 years with a slight male preponderance[1]. Because our study was started in the beginning of 2016, the diagnosis of the disease was made according to revised 2008 World Health Organization (WHO) PV diagnostic criteria [Table 1][2,3]. Revised 2016 WHO, PV criteria were also mentioned in Table 2 to point out the difference between the recent and former criteria[4].
Most patients with PV are diagnosed incidentally when an elevated hemoglobin or hematocrit is noticed on a complete blood count (CBC) obtained for some other reasons. Clinical manifestations of PV may vary from asymptomatic to various symptoms and findings such as headache, fatigue, sweating, itching, erythromelalgia, thrombosis, or hemorrhage.
Gastrointestinal complaints are common in PV, with a high incidence of epigastric distress, history of peptic ulcer, and gastroduodenal erosions on upper endoscopy[5]. Although the pathophysiology of gastrointestinal lesions in PV is unclear, altered gastric mucosal blood flow due to increased blood viscosity and/or increased histamine release from tissue basophils is thought to play a role in etiopathogenesis[6-10]. However, there are insufficient data on the frequency of HP and its role in etiopathogenesis. Only one study has reported a high incidence of positivity for infection with HP[5].
HP is a microaerophilic spiral-shaped Gram-negative microorganism that can be colonized in all parts of the stomach with gastric cell metaplasia, especially in antrum and corpus regions. These bacteria, infecting more than half of the world's population today, are a gastric pathogen that is the major cause of neoplastic and inflammatory gastroduodenal diseases. HP infection plays a major role in the etiology of peptic ulcer disease, atrophic gastritis, non-ulcer dyspepsia, gastric cancer, and mucosa-associated lymphoid tissue (MALT) lymphoma[11-13].
In this study, we aimed to compare the prevalence of HP infection in PV patients without dyspeptic complaints with a healthy control group without dyspeptic complaints. Thus, even if there is no dyspeptic complaint, the susceptibility to HP infection to be detected in PV patients, and the eradication treatment to be applied to this disease will decrease the incidence of gastric disorders and avoid expenses on these diseases in the future.
MATERIALS AND METHODS
Fifty PV patients diagnosed according to revised 2008 WHO criteria who admitted to hematology department in 2016 and as control group, 50 healthy volunteers who did not have dyspeptic complaints were enrolled in the study. Patients with previous therapy with H2-receptor antagonists, proton-pump inhibitors, HP eradication treatment before PV diagnosis, antibiotics within past 2 weeks, a history of gastroduodenal lesions, dyspepsia complaints, and patients under 18 years of age were excluded from the study.
Stool specimens of all patients and controls were tested with HP stool antigen (HPSA) test (True Line®) in our microbiology laboratory. HPSA test is a quick and qualitative test based on immunochromatography. Approximately 50 µg (almost ¼ of a green pea), stool was picked up by a sampling bar from the stool sample which was being held in a clean and dry sample vessel. This specimen was stirred with the buffer solution and four drops (0.15 mL) were dropped without any bubbles on the sample pool of the test case. It was evaluated according to the formation of red labels on both test and control areas in 10-15 min. In the presence of HP, a red label is formed as a result of an immunochromatographic reaction between HP antigens and colloidal latex particles covered by an antigenspecific monoclonal antibody. For positive results, red labels need to be formed on both control and test zones and that demonstrates HP antigen presence in the stool specimen. When a red label was formed on only control area, but not on test area, it was interpreted as negative result. Patients diagnosed with HP antigen positivity in stool were referred to the gastroenterology department for HP eradication treatment. Assent of both the patient and the control group was obtained using the informed consent form approved by the ethics committee.
Analysis of variance was used to compare control group and PV patients for HP antigen presence. T-test and Chisquare tests were used to evaluate the relationship between the hemogram parameters at the time of diagnosis, JAK2 V617F mutation presence, serum erythropoietin (EPO) level, splenomegaly presence on abdominal ultrasonography (USG), sex, age, and HP positivity in PV patients. Statistical analyses were performed with SPSS 21.0. (Statistical Package for the Social Sciences for Windows, Version 21.0., Chicago). Results were considered statistically significant at level P < 0.05.
RESULTS
In this study, 50 PV patients were included in the study. 74% (n = 37) of the PV patients were male, 26% (n = 13) were female, and the mean age was 53.18 ±15.04. 70% (n = 35) of the control group were male, 30% (n = 15) were female, and the mean age was 44.62 ± 15.82.
Fifty PV patients and 50 controls were compared in terms of presence of HP antigen; in PV group, 64% (n = 32) were HP positive and 36% (n = 18) were HP negative, whereas 2% (n = 1) of the control patients was HP positive and 98% (n = 49) was HP negative. HP infection was found significantly higher in PV patients than in controls (64% vs.2%) (P = 0.000).
Among PV patients, 61.5% (n = 8) of females and 64.7% (n = 24) of males were found to be positive for stool HP antigen. There was no significant difference between HP positivity in terms of sex (P = 0.830). And also, no statistically significant relationship was found between age groups and HP positivity in the PV patients (P = 0.250).
Thirty-eight of PV patients had JAK2 V617F mutation. Considering the relationship between the presence of JAK2 V617F mutation and HP positivity in PV patients, we found that while 24 of 38 JAK2 V617F mutation-positive PV patients had HP positivity, and 8 of 12 JAK2 V617F mutation-negative PV patients had HP positivity. There was no statistically significant correlation between JAK2 V617F mutation presence and HP positivity (P = 0.825).
In our study, 17 of the 26 PV patients with low serum EPO levels had positive HPSA and 9 had negative test results. Of the 24 patients with normal serum EPO levels, 15 were positive for HP and 9 for negative. There was no statistically significant relationship between serum EPO level and HP positivity (P = 0.832).
Among the PV group, splenomegaly (>11 cm) was found in 30 patients by abdominal USG examination, 19 of 30 patients were positive for HP and 11 were negative. Among 20 patients without splenomegaly, HP was found to be positive in 12 and negative in 8. Therefore, there was no statistically significant relationship between splenomegaly on USG and HP presence (P = 0.812).
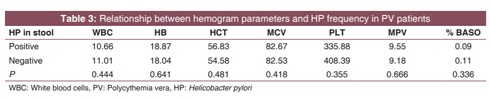
There was no statistically significant relationship between hemogram parameters of PV group at the time of diagnosis and HPSA positivity [Table 3].
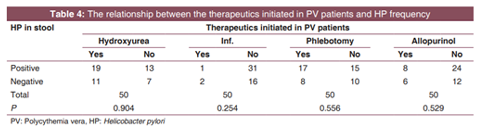
About 100% (n = 50) of PV patients were treated with acetylsalicylic acid (ASA), 60% (n = 30) with hydroxyurea, 50% (n = 25) with phlebotomy, 28% (n = 14) with allopurinol, and 6% (n = 3) with interferon-alpha. Relationship between HPSA positivity and treatment options was compared. There was no statistically significant relationship found between HP antigen positivity and treatments applied to PV patients [Table 4].
DISCUSSION
PV is a classical BCR-ABL-negative myeloproliferativeneoplasm characterized by clonal stem cell proliferation and a dysregulated JAK-STAT pathway. PV is primarily characterized by erythrocytosis and thrombocytosis, respectively. Other disease features include leukocytosis, splenomegaly, thrombohemorrhagic complications, vasomotor disturbances, pruritus, and a small risk of disease progression into acute myeloid leukemia or myelofibrosis[14].
In PV patients, peptic ulcer and gastroduodenal erosions are more common than the general population, with an average of 7-23%.[15-18] However, it is estimated that this value is normally lower due to the presence of subclinical cases and spontaneous regression. In fact, 70% of PV patients without dyspeptic complaints were found to have gastroduodenal damage with upper endoscopy[5].
Although the pathogenesis of gastrointestinal lesions in PV patients is not clearly known, it is thought that increased histamine secretion from basophils, gastric acid hypersecretion (hyperchlorhydria), hyperviscosity, and ischemia due to thrombosis of local mucosal vasculature is the reasons of increased peptic ulcer incidence and gastroduodenal erosions in PV patients.[6] However, most of these hypotheses are usually based on studies before HP identification. The data on the frequency of HP and its role in the pathogenesis of gastroduodenal lesions in PV are inadequate.
HP is a Gram-negative bacterium which causes chronic gastritis and plays important roles in peptic ulcer disease, gastric carcinoma, and gastric lymphoma. This bacterium is also associated with various other conditions including pulmonary, vascular, and autoimmune disorders[19,20]. Although 100% of HP infected people have gastritis histopathologically, most of them are asymptomatic. Dooley et al. have reported the prevalence of HP infection in asymptomatic individuals as 32%[21]. Only 30% of HP infected adults have dyspeptic symptoms. In patients with dyspeptic complaints, there is 20% risk for peptic ulcer development, 1-3% for gastric cancer, and 0.1% for primary gastric lymphoma. As a result, 20-30% of infected people may develop diseases such as duodenal ulcer, gastric ulcer, gastric carcinoma, and MALToma which may be life-threatening[22]. Various epidemiological studies have shown that at least 10% of asymptomatic carriers may develop symptomatic disease within the next 10 years and also at least 2-4% of symptomatic patients may develop gastric carcinoma within the next 10 years[19,20].
Until now, the number of studies investigating PV and HP, which seem to be independent from each other and may be associated with various pathophysiologic mechanisms, is scarce. The only study that searches for this possible association was reported by Torgano et al.[5] In this study, patients diagnosed with PV were examined endoscopically regardless of whether they had dyspeptic complaints or not, and gastritis, peptic ulcer, and HP positivity of the patients were investigated. These results were compared with endoscopy findings of the control group which had dyspeptic complaints, occult blood positive stool, and iron deficiency anemia. As a result, in PV patients, gastritis, peptic ulcer, and HP positivity were found to be significantly higher than the control group.
In our study, we also found that HP positivity was significantly higher in PV patients without dyspeptic complaints than asymptomatic healthy controls (64% vs. 2%). This result suggests that PV causes susceptibility to HP infection. The underlying mechanism is unclear. The gastric mucosa is protected from its own acid secretion and harmful microorganisms such as HP with various natural protection mechanisms. Among the mechanisms, the mucus-bicarbonate barrier comes first. The integrity of this barrier is protected by mucosal blood flow. Probably, this protection mechanism is disturbed, and the mucous membrane invasion of HP is facilitated since gastric mucosal blood flow slows down due to hyperviscosity of blood in the presence of PV. In addition, gastric acid hypersecretion due to increased histamine release in PV presence causes mucosal damage, facilitating HP mucosal invasion[23,24] However, more studies supporting thevalidity of these hypotheses are needed.
Patients without dyspeptic complaints were enrolled in this study because HP infection has high prevalence in developing countries (60-85%).[25] For our country, the most recent study of HP infection prevalence and risk factors in general population is TURHEP study that was completed in 2013[26]. In this study, involved 4622 people, the prevalence of HP infection was 82.5%. It is also expected that in patients with dyspeptic symptoms, the prevalence would be higher than asymptomatic individuals. Several studies using serological diagnostic tests have shown that HP positivity is lower in the normal population than in patients with dyspeptic complaints, although these studies are inadequate and out of date[27,28]. Therefore, it is not reasonable to investigate the increasing effect of a disease on the prevalence of this bacterium with such a high prevalence in our country, and it is more rational to include patients with no dyspeptic complaints, possibly with a lower prevalence of HP.
The ratio of HP seropositivity (2%) in our control group was really surprising even for us. In fact, there are only few studies investigating the prevalence of HP positivity in asymptomatic people. The most comprehensive one is performed by the EUROGAST Study Group[29]. They selected 3194 asymptomatic people and assayed their serum samples for the presence of anti-HP IgG antibodies. Finally, overall, 1563 (48.9%) people were found to be infected with HP. In a previously mentioned, relatively smaller sample size study, a lower HP prevalence in asymptomatic individuals which was 32% of 113 persons reported[21]. Even if the ratio of HP presence declines as sample sizes of the researches gets smaller, and there are not many studies on HP prevalence in asymptomatic individuals, we did not expect to encounter such a nominal result for HP prevalence in our control group. As designing our study, we could just simply report the HP prevalence in non-dyspeptic PV patients which was 64% and compare it with the one announced by the EUROGAST Study Group[29]. However, even though 50 control group cannot represent the whole asymptomatic population, we wanted to find it out again using the same HPSA test kits which were used for the group of PV patients. It was definitely unfortunate to come across only one individual with HP infection. According to our hypothesis, we have to compare the ratios of HP positivity in asymptomatic PV patients and controls with each other; but, it would be more revealing to compare our result demonstrating HP prevalence in asymptomatic PV patients with the ratio which was found in the most comprehensive investigation reported until now, including 3194 asymptomatic subjects[29].
The result of the primary outcome of our study was that HP frequency was significantly higher in the PV patients without dyspeptic complaints than in healthy individuals without dyspeptic complaints. The obvious difference (64% vs. 2%) between the two groups leads to the question of reliability of HPSA test. However, the same HPSA test was used in both groups, and it suggests that there is no technical error to cause this severe HP prevalence difference. In a study testing specificity and sensitivity of the HPSA, the results of test were compared with the histology and culture results. Sensitivity was found 98.2%, specificity was 93.1%, positive predictive value was 96.4%, and negative predictive value was 96.4%[30]. In a study conducted in our country, the sensitivity, specificity, positive predictive value, and negative predictive value of the HPSA test were 84%, 82%, 80%, and 86%, respectively[31]. In another current study, Schulz et al. used nine different screening tests in the follow-up of asymptomatic HP infected individuals. The HPSA test has been found to be the most cost-effective test to reduce the rates of peptic ulcer and gastric cancer[32].
In our study, we did not find significant relationship between HP positivity and age, gender, treatment modalities, CBC parameters at the time of diagnosis, presence of JAK2 V617F mutations, serum EPO level (low/normal-high), and splenomegaly in PV patients. This suggests that PV disease alone is an independent risk factor for the development of HP infection.
As a limitation of our study, we know that ASA must be included in the treatment of all PV diagnosed patients to prevent thrombotic complications unless there is a contraindication. All of our patients receive ASA therapy, and it is known that ASA decreases gastric mucosal protective factors such as prostaglandins by irreversibly inhibiting cyclooxygenase-1 and cyclooxygenase-2 enzymes. In this way, it may increase susceptibility to mucosal damage and HP colonization. It is difficult to say that the high HP positivity determined was whether due to the disease itself or ASA treatment since all PV patients in our study were under ASA treatment. It is not appropriate in terms of medical ethics and patient rights to discontinue current treatment and conducts a study in that way. A prospective study on HP scan, which can be performed before the initiation of treatment for PV may provide much more accurate conclusions regarding our hypothesis.
Another question that may come up in this study is the reason why we did not perform upper gastrointestinal system endoscopy to the patients included in the study. Contrary to other studies in the literature, we included asymptomatic PV patients who did not have any dyspeptic complaints. According to the Maastricht consensus published after the consensus meeting of the European HP Study Group in 2005 where the criteria for treatment and diagnosis of HP infections were determined; in developing countries, where HP infections are endemic, endoscopy is not recommended because of cost and time consumption for diagnosis, except for patients with alarm symptoms. It is recommended that diagnosis should be based on clinical findings and supported by non-invasive tests[33]. Although histopathologic examination is accepted as a gold standard in the diagnosis of HP infection, it is difficult to perform as an invasive screening test[34,35]. Thus, non-invasive methods such as serological tests, urea breath test, and HPSA test are used especially for screening or follow-up. For this reason, we used the HPSA test, which is non-invasive, with sensitivity and specificity >90% and can be used repeatedly without a reduction in reliability.
There may also appear a suspicion about the relatively low incidence of the presence of JAK2 V617F mutation, and the ratio of patients who have low serum EPO level. In our study, 38 of PV patients have JAK2 V617F mutation (76% n = 50) which is relatively lower than the ratio Tefferi et al. found in their study (98% n = 1545)[36]. There are also more studies that showed this ratio varied between 95% and 100% of patients with PV[37-39] In addition to this, the percentage of patients with low serum EPO level is 52% (26/50) which is lower than the ratio (81% n = 1545) stated in the same study of Tefferi et al[36]. The primary reason for these relatively low ratios is our limited sample size. It cannot be expected 50 patients to represent whole PV population. Besides that, in our clinic, JAK2 exon 12 mutation cannot be evaluated, and this obviously may lead the ratio of the presence of JAK2 mutation to be found relatively lower.
CONCLUSION
This is the first study on HP positivity in PV patients who do not have any dyspeptic complaints. Although 50 patients sample size is too limited for both PV patients and control group, this study and our hypothesis based on certain mechanisms help us to estimate the relationship between PV and HP. As a result, a non-invasive test such as HPSA test is required at least once for PV diagnosed patients even if there are no dyspeptic symptoms because HP screening and eradication are an effective strategy to reduce risks of gastric cancer and peptic ulcers development in HP high prevalence populations. Further studies with much larger sample size are warranted to determine the timing and applying frequency of this test for PV patients.
References
- Gilbert HS. The spectrum of myeloproliferative disorders. Med Clin North Am 1973;57:355-93.
- Spivak JL, Silver RT. The revised world health organization diagnostic criteria for polycythemia vera, essentialthrombocytosis, and primary myelofibrosis: An alternative proposal. Blood 2008;112:231-9.
- Tefferi A, Skoda R, Vardiman JW. Myeloproliferative neoplasms: Contemporary diagnosis using histology andgenetics. Nat Rev Clin Oncol 2009;6:627-37.
- Arber DA, Orazi A, Hasserjian R, Thiele J, Borowitz MJ, Le Beau MM, et al. The 2016 revision to the world healthorganization classification of myeloid neoplasms and acute leukemia. Blood 2016;127:2391-405.
- Torgano G, Mandelli C, Massaro P, Abbiati C, Ponzetto A, Bertinieri G, et al. Gastroduodenal lesions in polycythaemia vera: Frequency and role of helicobacter pylori. Br J Haematol 2002;117:198-202.
- Gilbert HS, Warner RR, Wasserman LR. A study of histamine in myeloproliferative disease. Blood 1966;28:795-806.
- Gray AG, Boughton BJ, Burt DS, Struthers GR. Basophils, histamine and gastric acid secretin in chronic myeloproliferative disorders. Br J Haematol 1982;51:117-23.
- Suzuki K, Konishi N, Tokura Y, Takigawa M. Telangiectasia macularis eruptiva perstans in polycythemia rubra vera. Eur J Dermatol 2002;12:201-3.
- Westin J, Granerus G, Weinfeld A, Wetterquist H. Histamine metabolism in polycythaemia vera. Scand J Haematol 1975;15:45-57.
- Valimaki M, Vuopio P, Salaspuro M. Plasma histamine and serum pepsinogen I concentrations in chronic myelogenous leukaemia. Acta Med Scand 1985;217:89-93.
- Baltrus DA, Amieva MR, Covacci A, Lowe TM, Merrell DS, Ottemann KM, et al. The complete genome sequence of helicobacter pylori strain G27. J Bacteriol 2009;191:447-8.
- Topley WW, William WC. Topley and Wilson's Microbiology and Microbial Infections. Bacteriology. 10th ed. Vol. 2. London: Hodder Arnold; 2005. p. 1563-1590.
- Graham DY. Campylobacter pylori and peptic ulcer disease. Gastroenterology 1989;96:615-25.
- Spivak JL, Barosi G, Tognoni G, Barbui T, Finazzi G, Marchioli R, et al. Chronic myeloproliferative disorders. Hematol Am Soc Hematol Educ Progr 2003;1:200-24.
- Wilbur DL, Ochsner HC. The association of polycythemia vera and peptic ulcer. Ann Intern Med 1935;8:1667.
- Videbaek A. Polycythaemia vera. Course and prognosis1. Acta Med Scand 2009;138:179-87.
- Calabresi P, Meyer OO. Polycythemia vera. I. clinical and laboratory manifestations. Ann Intern Med 1959;50:1182.
- Langman MJ, Cooke A. Gastric and duodenal ulcer and their associated diseases. Lancet 1976;307:680-3.
- Suerbaum S, Michetti P. Helicobacter pylori infection. N Engl J Med 2002;347:1175-86. Available from: http://www.nejm.org/doi/abs/10.1056/NEJMra020542. [Last cited on 2018 Jan 29].
- Bazzoli F, Bianchi Porro G, Bianchi MG, Molteni M, Pazzato P, Zagari RM, et al. Treatment of helicobacter pylori infection. Indications and regimens: An update. Dig Liver Dis 2002;34:70-83.
- Dooley CP, Cohen H, Fitzgibbons PL, Bauer M, Appleman MD, Perez-Perez GI, et al. Prevalence of helicobacter pylori infection and histologic gastritis in asymptomatic persons. N Engl J Med 1989;321:1562-6.
- Makola D, Peura DA, Crowe SE. Helicobacter pylori infection and related gastrointestinal diseases. J Clin Gastroenterol 2007;41:548-58.
- Kivilaakso E. High plasma HCO3-protects gastric mucosa against acute ulceration in the rat. Gastroenterology 1981;81:921-7.
- Starlinger M, Schiessel R. Bicarbonate (HCO3) delivery to the gastroduodenal mucosa by the blood: Its importance for mucosal integrity. Gut 1988;29:647-54.
- Toracchio S, Marzio L. Primary and secondary antibiotic resistance of helicobacter pylori strains isolated in central italy during the years 1998-2002. Dig Liver Dis 2003;35:541-5.
- Ozaydin N, Turkyilmaz SA, Cali S. Prevalence and risk factors of helicobacter pylori in Turkey: A nationally-representative,cross-sectional, screening with the 13C-Urea breath test. BMC Public Health 2013;13:1215.
- Wyatt JI, Dixon MF. Chronic gastritis--a pathogenetic approach. J Pathol 1988;154:113-24.
- Marshall BJ, Surveyor I. Carbon-14 urea breath test for the diagnosis of Campylobacter pylori associated gastritis. J Nucl Med 1988;29:11-6.
- Epidemiology of, and Risk Factors for, Helicobacter pylori Infection among 3194 Asymptomatic Subjects in 17 Populations. The EUROGAST Study Group. Gut 1993;34:1672-6.
- Us D, Hascelik G. Seroprevalence of Helicobacter pylori infection in an asymptomatic Turkish population. J Infect 1998;37:148-50.
- Aksoy DY, Aybar M, Ozaslan E, Kav T, Engin D, Ercis S, et al. Evaluation of the Helicobacter pylori stool antigen test (HpSA) for the detection of Helicobacter pylori infection and comparison with other methods. Hepatogastroenterology 2003;50:1047-9.
- Schulz TR, McBryde ES, Leder K, Biggs BA. Using stool antigen to screen for Helicobacter pylori in immigrants and refugees from high prevalence countries is relatively cost effective in reducing the burden of gastric cancer and peptic ulceration. Chakravortty D, editor. PLoS One 2014;9:e108610.
- Malfertheiner P, Megraud F, O'Morain C, Bazzoli F, El-Omar E, Graham D, et al. Current concepts in the management of Helicobacter pylori infection: The Maastricht III consensus report. Gut 2007;56:772-81.
- Zuniga-Noriega JR, Bosques-Padilla FJ, Perez-Perez GI, Tijerina-Menchaca R, Flores-Gutierrez JP, Garza HJ, et al. Diagnostic utility of invasive tests and serology for the diagnosis of Helicobacter pylori infection in different clinical presentations. Arch Med Res 2006;37:123-8. Available from:
http://www.linkinghub.elsevier.com/retrieve/pii/S0188440905002420. [Last cited on 2018 Jan 29] - Gomollon F, Ducons JA, Santolaria S, Omiste IL, Guirao R, Ferrero M, et al. Breath test is very reliable for diagnosis of Helicobacter pylori infection in real clinical practice. Dig Liver Dis 2003;35:612-8.
- Tefferi A, Rumi E, Finazzi G, Gisslinger H, Vannucchi AM, Rodeghiero F, et al. Survival and prognosis among 1545 patients with contemporary polycythemia vera: An international study. Leukemia 2013;27:1874-81. Available from: http://www. nature.com/articles/leu2013163. [Last cited on 2018 Jan 29].
- Wang YL, Vandris K, Jones A, Cross NC, Christos P, Adriano F, et al. JAK2 Mutations are present in all cases of polycythemia vera. Leukemia 2008;22:1289-9.
- Pardanani A, Lasho TL, Finke C, Hanson CA, Tefferi A. Prevalence and clinicopathologic correlates of JAK2 exon 12 mutations in JAK2V617F-negative polycythemia vera. Leukemia 2007;21:1960-3. Available from: http://www.nature. com/articles/2404810. [Last cited on 2018 Jan 29].
- Lasho TL, Pardanani A, Tefferi A. LNK Mutations in JAK2 Mutation-Negative Erythrocytosis. N Engl J Med 2010;363:1189-90