Evaluation of Kawasaki Disease Risk Scoring System in a Single Center Experience from Japan
Miho Ashiarai1, Asami Shinbo1, Kazuaki Matsumoto1, Hisae Nakatani1, Keiko Onda1, Mari Okada1, Masako Imai1, Natsuko Suzuki1, Akihiro Oshiba1, Masayuki Nagasawa1
Citation : Ashiarai M, Shinbo A, Matsumoto K, Nakatani H, Onda K, Okada M, Imai M, Suzuki N, Oshiba A, Nagasawa M. Evaluation of Kawasaki Disease Risk Scoring System in a Single Center Experience from Japan. Clin Res Pediatr 2018;1(1):1-5.
Kobayashi score (K-score) is widely accepted to predict intravenous immunoglobulin (IVIG) unresponsiveness in Kawasaki disease (KD) and used for treatment stratification. However, its efficacy has been argued by the reports from Western countries.
From 2013 to 2016, K-score was evaluable in 209 of 225 newly diagnosed Japanese KD patients in our institute. Among them, 16 patients were treated with only acetylsalicylic acid, and 172 patients were initially treated with IVIG (2 g/kg). IVIG unresponsiveness was observed in 33 of 130 patients (25.4%) with K-score <5, and in 16 of 42 patients (38.1%) with K-score =5, yielding sensitivity of 32.7%, and specificity of 78.9%. 21 patients with K-score =5 were initially treated with IVIG + prednisolone (PSL; 2 mg/kg/day), and four patients showed unresponsiveness. Coronary artery aneurysm was observed in five patients with K-score <5, in which three were unresponsive to initial IVIG, and in one patient with K-score =5, who was unresponsive to IVIG + PSL.
K-score system has good specificity, but low sensitivity for predicting IVIG unresponsiveness and further modification is required.
Intravenous immunoglobulin unresponsiveness, Kawasaki disease, Kobayashi score.
INTRODUCTION:
Kawasaki disease (KD) is an acute inflammatory disease with unknown etiology which is diagnosed based on six main clinical symptoms and develops mostly in infants <4 years old [1,2]. The prevalence of KD differs substantially among countries, with the highest incidence in Japan, which is 10-20-fold of Western countries [3].
Coronary artery aneurysm (CAA) during the acute phase is well known as serious complication [3]. Although the precise long-term prognosis of CAA is to yet be determined, it is believed to cause acute myocardial ischemia or infarction eventually and the subsequent sudden death in some cases [4]. The incidence of CAA has been decreased from 20% to <3% dramatically through the early introduction of intravenous immunoglobulin (IVIG) (2 g/kg) therapy in combination with oral acetylsalicylic acid (ASA) (30 mg/kg/day) during the past three decades [3,5]. Recently, targeting therapy to tumor necrosis factor alpha has been shown effective to refractory KD [6].
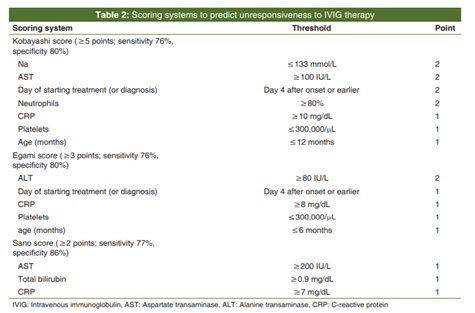
After efficacy of the treatment by IVIG has been established with the subsequent dramatic decrease of CAA complications, several severity classifications for IVIG unresponsiveness as substitution endpoints for CAA complications are applied to further improve the clinical outcome [3]. Among them, Japanese Kobayashi score (K-score) [7], Egami score (E-score) [8], and Sano score (S-score)[9] system are well known and have been reported useful to predict IVIG unresponsiveness [Table 1]. The K-score uses 7 factors whereas E-score and S-score use 5 and 3 factors, respectively [7-9]. The factors adopted in three classifications are almost overlapping, except for total bilirubin level adopted in S-score.
Recently, K-score is widely accepted because treatment stratification with K-score has shown the significant effectiveness in the large prospective clinical study in Japan [10]. However, the usefulness and effectiveness of K-score system have been argued by the reports from UK[11] and USA [12].
We report a clinical experience of Japanese KD patient in our institute and discuss the clinical problem with K-score system.
PATIENTS AND METHODS:
We experienced 225 newly diagnosed KD patients in our institute between 2013 and 2016.
Of 225 patients, K-score was evaluable in 209 cases. The details of the patients are presented in Table 2. Principally, the initial treatment was carried out with IVIG (2 g/kg) + ASA (30 mg/kg/day), and 16 cases with mild symptoms were treated with only ASA. We conducted prednisolone (PSL) combination in addition to IVIG + ASA for cases with K-score of five points or more from June 2016, according to the report.
In summary, IVIG + ASA was applied for 188 patients, IVIG + ASA + PSL (2 mg/kg/day) for 21 patients, and ASA for 16 patients, as an initial treatment.
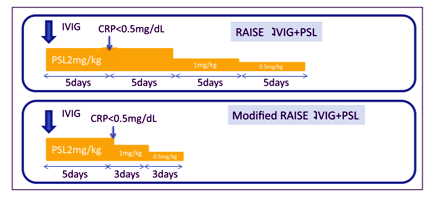
We modified the way of PSL tapering. Briefly, PSL (2 mg/kg/day) was given at least for 5 days and decreased after C-reactive protein (CRP) <0.5 mg/dL was confirmed. Subsequently, PSL (1 mg/kg/day) was given for 2-3 days and PSL (0.5 mg/kg/day) for 2-3 days [Figure 1].
Unresponsive to IVIG + ASA therapy was defined as follows; the decline of fever (<37.5°) was not obtained, or fever was re-increased again more than 37.5° within 24-36 h after IVIG injection.
Statistical analysis was performed using a Chi-square method and P < 0.05 was considered as statistically significant.
RESULTS:
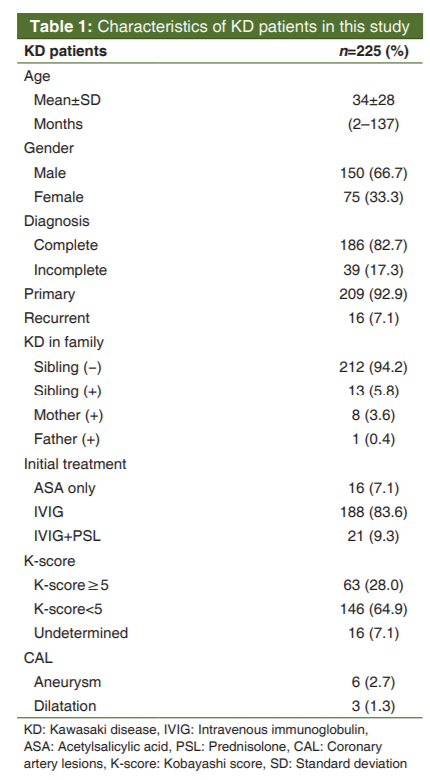
Of 225 patients, 150 were male (66.7%), and the mean age was 34 months (range 2-137 months) with a median of 25 months. The treatment was started from 1st to 9th day, with a mean of 4.8 ± 1.3 days (median of the 5th day). 16 cases were recurrent, and siblings had a history of KD in 13 cases. In nine cases, either parent had a history of KD. Concerning with diagnosis, 186 cases were complete, and 39 cases were incomplete. CAA was observed in 6 cases (2.7%), and dilatation in 3 cases (1.3%).
For a refractory case to the initial treatment or a case with re-fever, IVIG repeated dose, IVIG repeated dose + PSL combination, or methylprednisolone pulse therapy were provided.
Infliximab was given in two refractory cases, in one of which giant aneurysm developed.
Then, we performed analysis for 209 cases, in which K-score at diagnosis was evaluable [Figure 2].
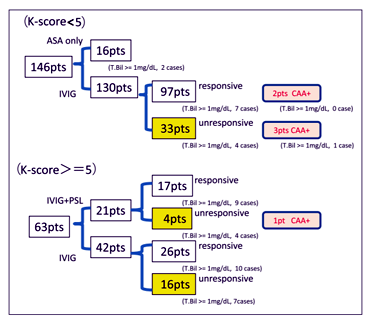
K-score was five points or more in 63 cases (30.1%). In 146 cases with <5 points, 16 cases were treated with only ASA and healed without a relapse and coronary artery lesions. 130 patients received initial IVIG therapy; 97 patients responded and 33 cases (25.4%) were unresponsive. 42 of 63 patients with five points or more received initial IVIG, and 21 patients received IVIG + PSL combination therapy. 26 patients responded among the former, and 16 cases (38.1%) were unresponsive. 17 patients responded among the latter, and 4 cases (19.0%) were unresponsive.
We examined an unresponsiveness prediction by K-score about 172 patients who received initial IVIG treatment. A Chi-square test presented no significance (odds ratio = 1.81, 95% confidence interval [CI]: 0.87-3.78, P = 0.11), and sensitivity and specificity for unresponsiveness prediction were 32.7% and 78.9%, respectively.
The CAA was found in one unresponsive case for IVIG + PSL treatment, and in 5 cases with K-score of <5.
In 21 cases treated with IVIG + PSL, a mean period of PSL administration was 10.7 days with 2 mg/kg/day for 5.9 days (5-8 days) and 1-0.5 mg/kg for 4.8 days (3-6 days). There was no relapse during the PSL tapering, and a mean PSL administration period of 10.7 days was much less than minimum 20 days of original RAISE study method [10].
DISCUSSION:
Our report from a Japanese single institute also exhibited similar results as those of the reports from UK [11] and USA [12], which argued the efficacy of K-score system. In particular, the sensitivity in our study was as low as 32.7%, which was much worse than 76% in the original report [7].
In 172 patients who received IVIG + ASA as an initial treatment, 33 cases in a group of K-score <5 (33/130 = 0.254) and 16 cases in the K-score =5 group (16/42 = 0.38) showed IVIG unresponsiveness, and there was no significant difference between both groups (odds ratio = 1.81, 95% CI: 0.87-3.78, P = 0.11). CAA developed in one case of K-score =5 group (1/42 = 0.024), and in 5 cases of K-score <5 group (5/130 = 0.038), which exhibited no significant difference (odds ratio = 0.69, 95% CI: 0.07-5.37, P = 0.65). About K-score =5 group, 16 of 42 cases with IVIG treatment (16/42 = 0.381) and 4 of 21 cases with IVIG + PSL treatment (4/21 = 0.190) showed unresponsiveness to initial treatment, which showed difference (odds ratio = 2.62, 95% CI: 0.75-9.17, P = 0.13), although not statistically significant. It was thought that the treatment escalation by PSL addition was feasible for K-score =5 groups.
Based on these observations, prediction of IVIG unresponsiveness by K-score should be reconsidered. Particularly, it should be emphasized that more than expected IVIG unresponsive cases were still involved in the low K-score group. It seems important to find a new factor to predict IVIG unresponsiveness in a case of the K-score <5 group.
In this regard, we have found that a D-dimer level may be useful as one candidate factor (submitted). KD is classified as medium vessel vasculitis pathologically [13], and D-dimer is regarded as a useful indicator of vasculitis [14]. Furthermore, it has been reported that elevated D-dimer is related with severity of KD [15,16]. Briefly, IVIG unresponsiveness prediction by K-score is effective in the case with D-dimer <2.5 μg/mL, whereas it is more likely to be IVIG unresponsive in the case with D-dimer =2.5 μg/mL, even if with low K-score.
In the original report of RAISE study [10], PSL (2 mg/kg/day) was further continued for 5 days after having confirmed CRP <0.5 mg/dL, 1 mg/kg/day, and 0.5 mg/kg/day of PSL was given for 5 days, respectively, during the tapering, which resulted in minimum of 20 days PSL administration.
In our practice, total PSL administration period was reduced to 10.7 days, which was almost half of 20 days. Considering the adverse effects of the long-term PSL administration, our method seems feasible enough.
As mentioned previously, total bilirubin level (T-Bil) is involved in S-score, but not in K-score and E-score. We examined the impact of bilirubin level on K-score system.
In the cases with K-score <5, T-Bil was 1mg/dL or more in four of 33 cases (12.1%) with IVIG unresponsiveness and in 13 of 146 cases (8.9%) with IVIG responsiveness, whereas, T-Bil was 1 mg/dL or more in 30 of 63 cases (47.6%) with K-score =5. However, T-Bil was 1mg/dL or more in 7 of 16 cases (43.8%) with IVIG unresponsiveness, and in 10 of 26 cases (38.5%) with IVIG responsiveness among K-score =5 groups, which showed no significant difference. In 21 cases who received IVIG + PSL, T-Bil was 1 mg/dL or more in 9 of 17 cases (52.9%) with responsiveness, and in all of 4 cases (100%) who presented unresponsiveness to IVIG + PSL treatment [Figure 2].
T-Bil is used for a severity classification with S-score[9], and it is easily expected that it is closely related with severity of KD determined by K-score. However, it is uncertain whether T-Bil is useful as an additional factor to predict more severe KD who presents IVIG + PSL unresponsiveness in the case with K-score =5.
CONCLUSION:
K-score system has good specificity (78.9%) but low sensitivity (32.7%) for predicting IVIG unresponsiveness in our cohort. Our patients were all Japanese, and the discrepancy between original report of Japan and those of UK and USA could not be attributed to racial differences. Further modification is necessary to improve the sensitivity of the scoring system to predict IIG unresponsiveness of KD.
MA and MN designed this study, analyzed the data and drafted the manuscript. MA, AS, KM, HN, KO, MO, MI, NS and AO were involved in patient management and collected the clinical data. MN reviewed the literature and gave a final approval of the manuscript.
This study is approved by the Institutional Review Board and informed consent is secured by opt-out method.
Authors have no funding concerning with this study.
Authors have no conflict of interest to declare.
References
- Kawasaki T, Kosaki F, Okawa S, Shigematsu I, Yanagawa H. A new infantile acute febrile mucocutaneous lymph node syndrome (MLNS) prevailing in Japan. Pediatrics 1974;54:271-6.
- Cohen E, Sundel R. Kawasaki disease at 50 years. JAMA Pediatr 2016;170:1093-9.
- Group JJ. Guidelines for diagnosis and management of cardiovascular sequelae in Kawasaki disease (JCS 2013). Digest version. Circul J 2014;78:2521-62.
- Wei YJ, Zhao XL, Liu BM, Niu H, Li Q. Cardiac complications in 38 cases of kawasaki disease with coronary artery aneurysm diagnosed by echocardiography. Echocardiography (Mount Kisco, Ny) 2016;33:764-70.
- Kuo HC. Preventing coronary artery lesions in Kawasaki disease. Biomed J 2017;40:141-6.
- Mori M, Imagawa T, Hara R, Kikuchi M, Hara T, Nozawa T, et al. Efficacy and limitation of infliximab treatment for children with Kawasaki disease intractable to intravenous immunoglobulin therapy: Report of an open-label case series. J Rheumatol 2012;39:864-7.
- Kobayashi T, Inoue Y, Takeuchi K, Okada Y, Tamura K, Tomomasa T, et al. Prediction of intravenous immunoglobulin unresponsiveness in patients with Kawasaki disease. Circulation 2006;113:2606-12.
- Egami K, Muta H, Ishii M, Suda K, Sugahara Y, Iemura M, et al. Prediction of resistance to intravenous immunoglobulin treatment in patients with Kawasaki disease. J Pediatr 2006;149:237-40.
- Sano T, Kurotobi S, Matsuzaki K, Yamamoto T, Maki I, Miki K, et al. Prediction of non-responsiveness to standard high-dose gamma-globulin therapy in patients with acute Kawasaki disease before starting initial treatment. Eur J Pediatr 2007;166:131-7.
- Kobayashi T, Saji T, Otani T, Takeuchi K, Nakamura T, Arakawa H, et al. Efficacy of immunoglobulin plus prednisolone for prevention of coronary artery abnormalities in severe Kawasaki disease (RAISE study): A randomised, open-label, blinded-endpoints trial. Lancet (London, England) 2012;379:1613-20.
- Davies S, Sutton N, Blackstock S, Gormley S, Hoggart CJ, Levin M, et al. Predicting IVIG resistance in UK Kawasaki disease. Arch Dis Childhood 2015;100:366-8.
- Sleeper LA, Minich LL, McCrindle BM, Li JS, Mason W, Colan SD, et al. Evaluation of Kawasaki disease risk-scoring systems for intravenous immunoglobulin resistance. J Pediatr 2011;158:831-5e3.
- Newburger JW, Takahashi M, Burns JC. Kawasaki disease. J Am Coll Cardiol 2016;67:1738-49.
- Hergesell O, Andrassy K, Nawroth P. Elevated levels of markers of endothelial cell damage and markers of activated coagulation in patients with systemic necrotizing vasculitis. Thromb Haemost 1996;75:892-8.
- Imamura T, Yoshihara T, Yokoi K, Nakai N, Ishida H, Kasubuchi Y. Impact of increased D-dimer concentrations in Kawasaki disease. Eur J Pediatr 2005;164:526-7.
- Masuzawa Y, Mori M, Hara T, Inaba A, Oba MS, Yokota S. Elevated D-dimer level is a risk factor for coronary artery lesions accompanying intravenous immunoglobulin-unresponsive Kawasaki disease. Ther Apher Dial 2015;19:171-7.