Blunt Trauma of a Horseshoe Kidney: Diagnosis Made on a Computed Tomography
Tenkorang Somuah, Sow Aboubakry, Ahsaini Mustapha, Mellas Soufiane, El Ammari Jalal Eddine, Tazi Mohammed Fadl, El Fassi Mohammed Jamal, Farih Moulay Hassan
Citation : Somuah T, Aboubakry S, Mustapha A, Soufiane M, Eddine EAJ, Fadl TM, Jamal EFM, Hassan FM. Blunt Trauma of a Horseshoe Kidney: Diagnosis made on a computed tomography. Clin Res Urol 2018;1(1):1-3.
The horseshoe kidney is a relatively rare congenital anomaly. The fortuitous discovery of a horseshoe kidney during radiological investigation in the event of an abdominal trauma is exceptional. Computed tomography plays a major diagnostic role in emergency units allowing appropriate and immediate patient care and follow-up. We report the case of a horseshoe kidney trauma that evolved well through a conservative approach.
Computed tomography, horseshoe kidney, trauma
INTRODUCTION
The horseshoe kidney is a rare congenital anomaly characterized by a renal fusion [1,2]. The discovery of a horseshoe kidney is most often fortuitous during radiological imaging for various etiologies including abdominal trauma [3,4]. We report a case of a ureter rupture in a horseshoe kidney diagnosed during computed tomography (CT) scan in the event of an abdominal trauma. The purpose of this study is to describe the contribution of a CT scan in diagnosing a non-surgical horseshoe kidney in a blunt abdominal trauma.
CASE REPORT
A Moroccan male of 21 years old with no history of any significant disease was transferred to our emergency department for the management of a post-traumatic hematuria.
This was a blunt abdominal trauma that had occurred 24 h before his admission to the emergency department. He complained of a total gross hematuria containing blood clots associated with an abdominal pain. Physical examination found a patient in a good general condition with diffuse abdominal sensitivity accentuated at the epigastric region, ecchymosis of the right hypochondrium.
Laboratory investigations revealed a normal serum creatinine at 10 μmol/L, urea at 0.47 mg/ml, hemoglobin level at 10.1 g/dL, leukocytosis at 10210/mm3,elevated C-reactive protein at 356 mg/l, and platelets at 171 103/uL.
An ultrasound had already been performed for the patient. It had objectified an intraperitoneal effusion of medium abundance slightly hyperechoic in nature, without any sign of visceral injury.
The patient took an emergency abdominal CT scan. A triphasic protocol was used as follows: An early arterial phase (20 s), a portal phase (120 s), and a delayed phase (15 min), for a better post-traumatic injury evaluation.
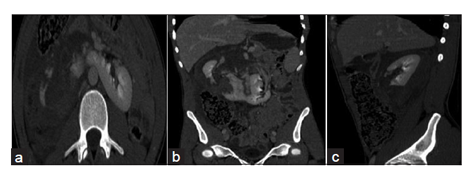
The CT scan objectified a malformative anomaly of the kidneys characterized by a fusion of the two kidneys connected at their lower poles suggestive of a horseshoe kidney.
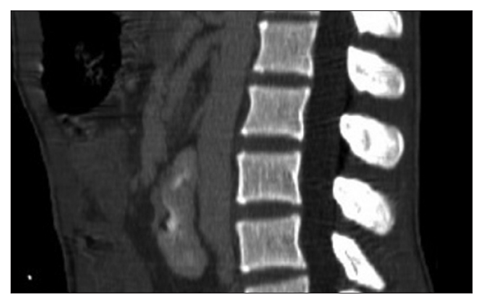
The portal phase of the CT scan showed the presence of a posterior medial corticomedullary fracture, accompanied by a retroperitoneal hematoma extending into the intraperitoneal cavity [Figure 1]. The horseshoe fusion was located below the lower mesenteric artery, and there was no post-traumatic vascular injury [Figure 2].
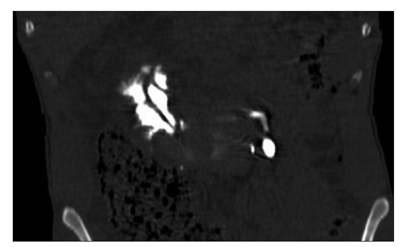
The delayed phase revealed a localized extra urinary leakage of the contrast material at the midlower calyces [Figure 3].
According to the American Association for the Surgery of Trauma (AAST) classification, our patient�s injury correlates with a deep fracture extending to the excretory system (urinary leak). This would be a Grade IV or Stage III in the classification of Chatelain [5].
A non-operative treatment was instituted after a multidisciplinary consultation. A JJ stent was placed. The urethra appeared normal during the procedure.
The patient evolved very well with no complications.
Radiological follow-up of the patient comprising ultrasounds and computed tomography (CT) scan was carried out.
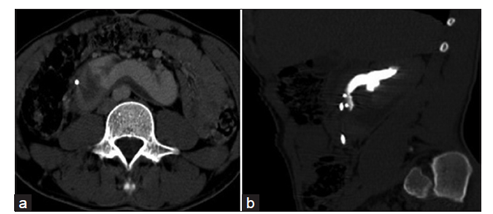
Quarterly CT scan monitoring showed total hematoma regression in the perirenal space and no extravasation of contrast material at the delayed phase. Nevertheless, a small devascularized fragment was observed on the right posterior renal hilar lip [Figure 4].
DISCUSSION
Our illustration reinforces the usefulness of a CT scan in deciding against surgery on a horseshoe kidney in the event of a blunt abdominal trauma.
The horseshoe kidney remains the most common form of renal fusion, anomalies affecting 1/400-1/1000 with a slightly predominance in men [1]. It would appear that the fusion of the two metanephrogenic blastemas occurring embryologically between the 4th and the 8th week of embryonic life can occur at different periods, leading to anomalies of ascension, rotation, and vascularization of the connected kidneys [6].
The fusion of the kidneys affects the lower poles in 96% of cases. "Horseshoe" kidney is most often located in front of large vessels below the origin of the lower mesenteric artery [1,7].
It is frequently discovered in the event of a complication, or incidentally during radiological imaging of another disease or a trauma,[1] as it was in our case.
Ultrasound screening is delicate, except for newborns [1]. CT scan with a four-phase acquisition is the best initial imaging modality in the management of any abdominal trauma [1,8-12]. The data obtained from the CT scan aid to evaluate the severity of renal traumas with the help of the classifications by AAST or by Chatelain [5]. In our case, the fracture line concerned the posterior medial corticomedullary region associated with a urohematoma; it correlates with that of an AAST Grade IV or a Chatelain Type III, without any injury to the isthmus of the horseshoe kidney.
The management of kidney trauma depends on the hemodynamic state of the patient and the associated injuries. Conservative treatment is sufficient for the vast majority of blunt kidney trauma [4,7,13]. Conservative treatment was maintained as our patient was stable despite the presence of a large urohematoma. This attitude can be prudently taken so long as it is not a Chatelain Grade V injury, as kidney injuries alone rarely lead to hemodynamic instability [14]. In addition, isolated urinary leaks regress spontaneously in about 80% of cases and should not be operated [14]. In all cases, radiological monitoring is required for these patients and urine drainage may be induced by placing a percutaneous nephrostomy or JJ stent in case of persistent urinary leakage, urinoma, or infection [15,16].
The 2004 International Consensus Conference recommends that an AAST Grade 4 injury requires CT scan monitoring at 36 and 72 h, with a late phase acquisition in search of associated injuries to the ureter [9]. In our case, the follow-up of the patient was unremarkable.
CONCLUSION
Blunt abdominal trauma on a horseshoe kidney is rare. Four-phase CT scan is the best imaging modality to classify any occurring injury to establish an appropriate therapeutic method. Non-operative approach is currently the preferred therapeutic option, but this depends on the hemodynamic state of the patient.
REFERENCES
- Veyrac C. Anomalies congenitales du rein et de la voie excretrice superieure chez l'enfant. Encycl Med Chir 2004;34:10.
- Averous M, Veyrac C. Malformations congenitales du rein. Encycl Med Chir Urol 1995;18-125-A10:9.
- Bordei P, Stantohe D, Iliescu D, Sapte E. Ectopic horseshoe kidney. A case report. Surg Radiol Anat 2004;26:474-9.
- Kontogeorgos L. Rupture traumatique de l'isthme d'un rein en fer a cheval. J Urol Nephrol (Paris) 1977;83:821-4.
- Escudero RM, Gil MJ, Alonso AH, Garcia EL, Amo FH, Pinies GO, et al. Traumatic rupture of horseshoe kidney. Urol Int 2012;88:112-14.
- Samison LH, Ferretti L, Rakotoaijaona AH, Tauzin C, Laborde Y. Rupture isthmique complete post-traumatique d'un rein en fer a cheval. Prog Urol 2006;16:201-3.
- Daudia A, Hassan TB, Ramsay D. Trauma to a horseshoe kidney. J Accid Emerg Med 1999;16:455-6.
- Sandler CM, Amis ES Jr., Bigongiari LR, Bluth EI, Bush WH Jr., Choyke PL, et al. Diagnostic approach to renal trauma. American college of radiology. ACR appropriateness criteria. Radiology 2000;215:727-31.
- Santucci RA, Wessells H, Bartsch G, Descotes J, Heyns CF, McAninch JW, et al. Evaluation and management of renal injuries: Consensus statement of the renal trauma subcommittee. BJU Int 2004;93:937-54.
- Hagiwara A, Sakaki S, Goto H, Takenega K, Fukushima H, Matuda H, et al. The role of interventional radiology in the management of blunt renal injury: A practical protocol. J Trauma 2001;51:526-31.
- Bretan PN Jr., McAninch JW, Federle MP, Jeffrey RB Jr. Computerized tomographic staging of renal trauma: 85 consecutive cases. J Urol 1986;136:561-5.
- Yao DC, Jeffrey RB Jr., Mirvis SE, Weekes A, Federle MP, Kim C, et al. Using contrast-enhanced helical CT to visualize arterial extravasation after blunt abdominal trauma: Incidence and organ distribution. AJR Am J Roentgenol 2002;178:17-20.
- Wein AJ, Murphy JJ, Mulholland SG, Chait AW, Arger PH. A conservative approach to the management of blunt renal trauma. J Urol 1977;117:425-7.
- McGahan JP, Richards JR, Jones CD, Gerscovich EO. Use of ultrasonography in the patient with acute renal trauma. J Ultrasound Med 1999;18:207-13.
- McAninch JW, Carroll PR, Klosterman PW, Dixon CM, Greenblatt MN. Renal reconstruction after injury. J Urol 1991;145:932-7.
- Moudouni SM, Hadj Slimen M, Manunta A, Patard JJ, Guiraud PH, Guille F, et al. Management of major blunt renal lacerations: Is a nonoperative approach indicated? Eur Urol2001;40:409-14.